
Central Nervous System (CNS)
&
Cranial Nerves
.. …… 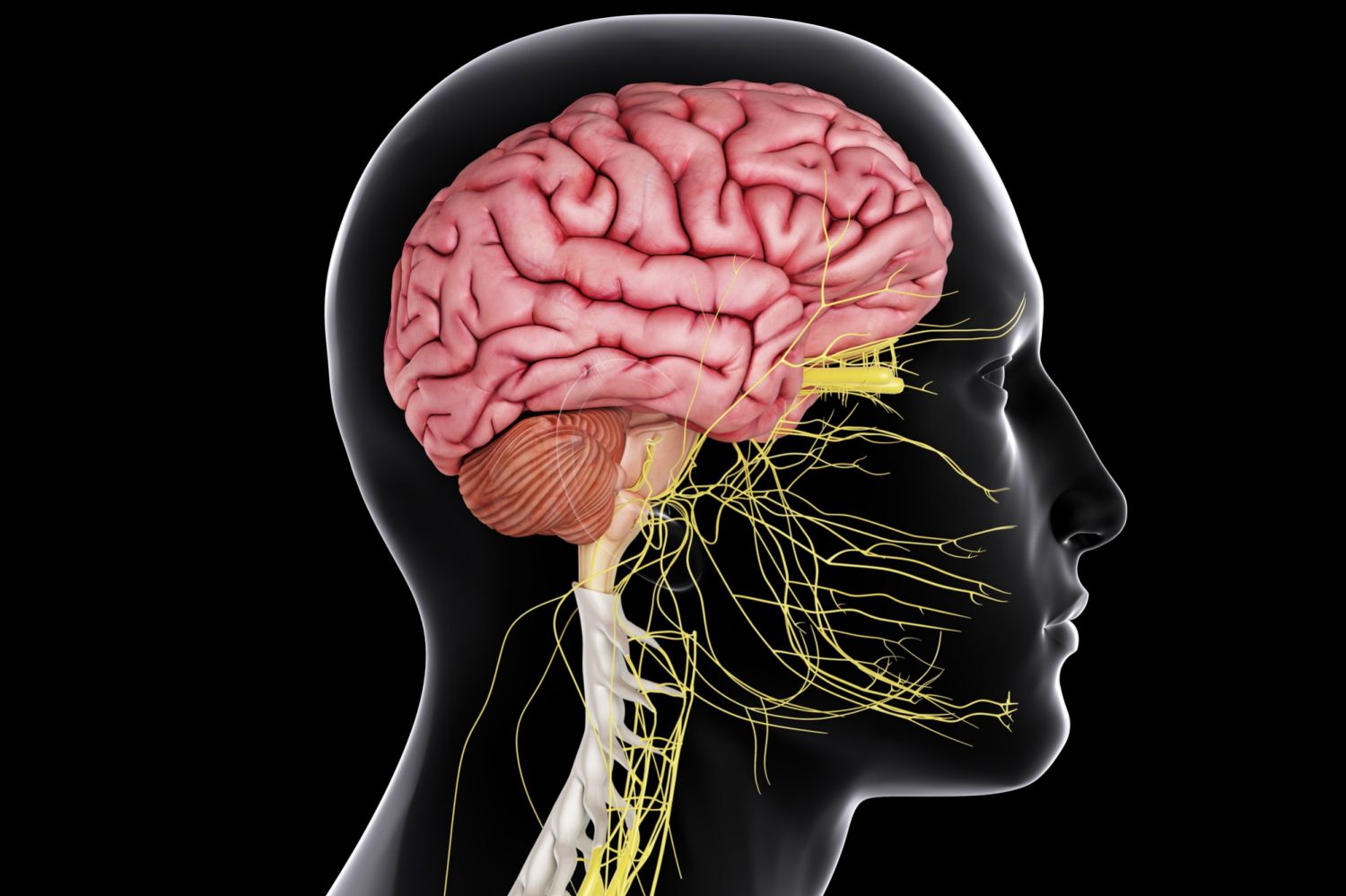
The CNS consists of the brain and spinal cord. They are enveloped and protected by three layers of meninges and encased within the skull and vertebral column. The brain consists of the cerebrum, subcortical structures, brainstem, and cerebellum.
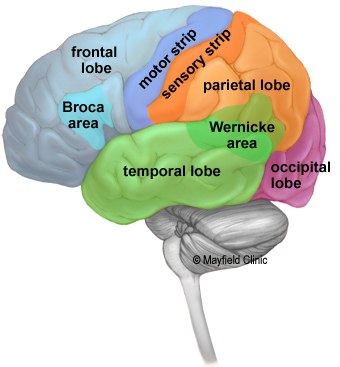
The cerebrum is the most prominent part of the brain. It consists of two cerebral hemispheres interconnected by the corpus callosum. The surface of the cerebrum is composed of sulci (ridges) and gyri (folds). This is where the highest processing power and cognitive ability in the entire nervous system takes place.
Each hemisphere is composed of 4 lobes: Frontal, Parietal, Temporal, Occipital.
LOBES
1. Frontal Lobe
The frontal lobe is considered our behavior and emotional control center and home to our personality. The frontal lobe is responsible for voluntary movement, expressive language and for managing higher level executive functions such as problem solving, judgement, spontaneity, initiation, impulse control, and social and sexual behavior. Located within the frontal lobe are the motor cortex and Broca’s area which controls motor functions responsible for producing language.
2. Parietal Lobe
The parietal lobe is responsible for processing sensory information and contains the somatosensory cortex. Neurons in the parietal lobe receive information from sensory and proprioceptors throughout the body.
3. Occipital Lobe
The occipital lobe, known as the visual processing center, contains the visual cortex. The occipital lobe receives information from the retina and then uses past visual experiences to interpret and recognize the stimuli.
4. Temporal Lobe
The temporal lobe processes auditory stimuli through the auditory cortex. Mechanoreceptors located in the hair cells
lining the cochlea are activated by sound energy, which in turn sends impulses to the auditory cortex.
The Wernicke area is in the temporal lobe and functions in speech comprehension.
SUBCORTICAL STRUCTURES
The subcortical structures are a neural group of structures embedded deep within the brain. They include the diencephalon, basal ganglia, limbic system, and pituitary gland.
Diencephalon 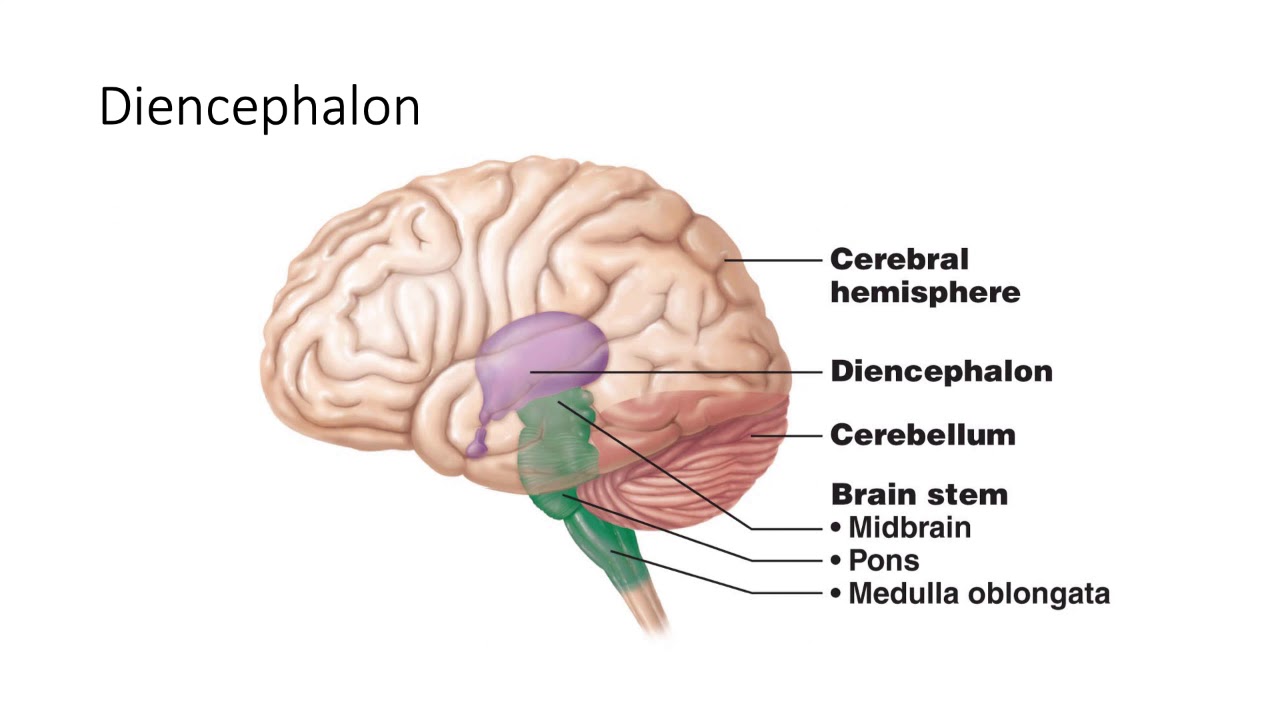
The diencephalon can be found just above the brainstem between the cerebral hemispheres. Although it is a relatively small part of the CNS in terms of mass, the diencephalon has a number of critical roles in healthy brain and bodily function.
The diencephalon is a collection of four cerebral structures that include:
I. Thalamus
The thalamus relays sensory and motor information to and from the cerebral cortex.
II. Epithalamus
The function of the epithalamus is to connect the limbic system to other parts of the brain. The pineal gland is part of the epithalamus and secretes the hormone melatonin which plays an important role in the regulation of circadian rhythms (sleep-wake cycle).
III. Subthalamus
The somatosensory fibers pass through the subthalamus and modulates movement. The role of the subthalamus is in the control, integration and accuracy of motor activity. A portion of the subthalamus is made up of tissue from the midbrain extending into the diencephalon. It contains the subthalamic nucleus which is interconnected with the basal ganglia and has many connections throughout the cortex and spinal cord.
IV. Hypothalamus
The hypothalamus’ most basic function is homeostasis (maintaining a steady internal state). It plays a key role in linking the nervous system to the endocrine system via the pituitary gland, influencing hormone release. The hypothalamus is involved in mediating endocrine, autonomic, visceral, and homeostatic functions. The hypothalamus receives a large amount of input from limbic structures. It has a large part to play in the homeostasis of many physiological systems such as hunger, thirst, water and sodium balance and temperature regulation. It regulates the stress response, metabolism and reproduction and plays a role in memory and emotional responses.
Limbic System
The limbic system is a complex set of brain structures that play a crucial role in emotions, motivation, learning, and memory. It is sometimes referred to as the “emotional brain” or “emotional center” of the brain. The limbic system is not a distinct anatomical structure but rather a collection of interconnected structures and networks that work together to regulate various emotional and behavioral responses. The limbic system works in conjunction with other brain regions to regulate emotional responses and behaviors. The limbic system allows for complex interactions between the cortex, the thalamus, the hypothalamus, and the brainstem.
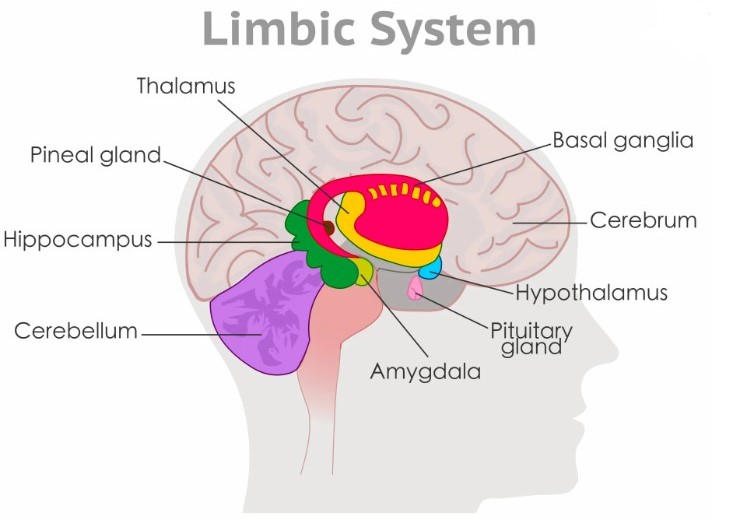
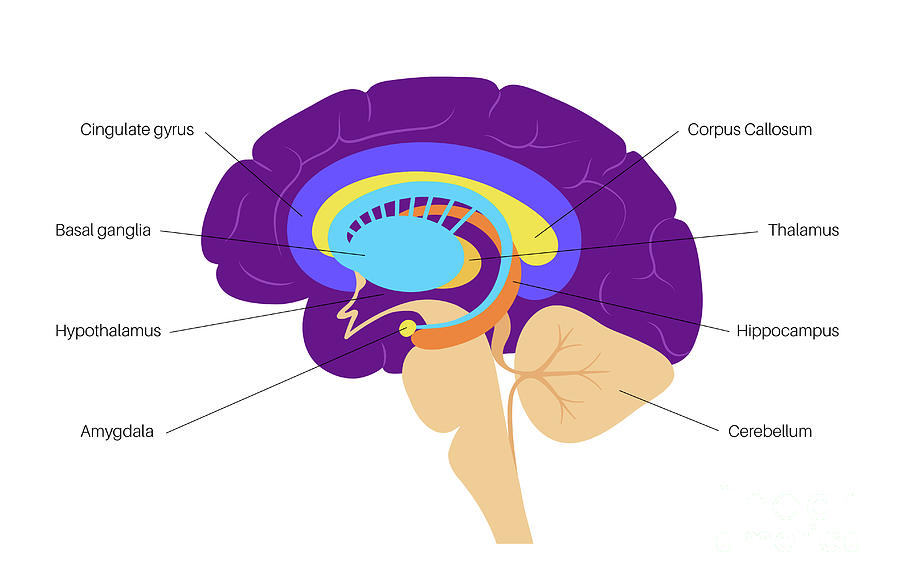
Key components of the limbic system include:
Hypothalamus: Refer to info above
Thalamus: Refer to info above
Hippocampus: This structure is essential for the formation of new memories and the consolidation of short-term memories into long-term memories. It is also involved in spatial navigation.
Amygdala: The main function of the amygdala is in emotional responses, including feelings of happiness, fear, anger, and anxiety. The amygdala is critical for processing emotions, especially fear and pleasure. It plays a role in the formation and storage of emotional memories and is involved in the body’s fight-or-flight response. The amygdala interacts with the hippocampus by attaching emotional content to memories and is therefore, also key for the formation of new memories.
Cingulate gyrus: This area is believed to help regulate emotions, behavior, and pain. It is also involved in predicting and avoiding negative consequences.
Basal Ganglia 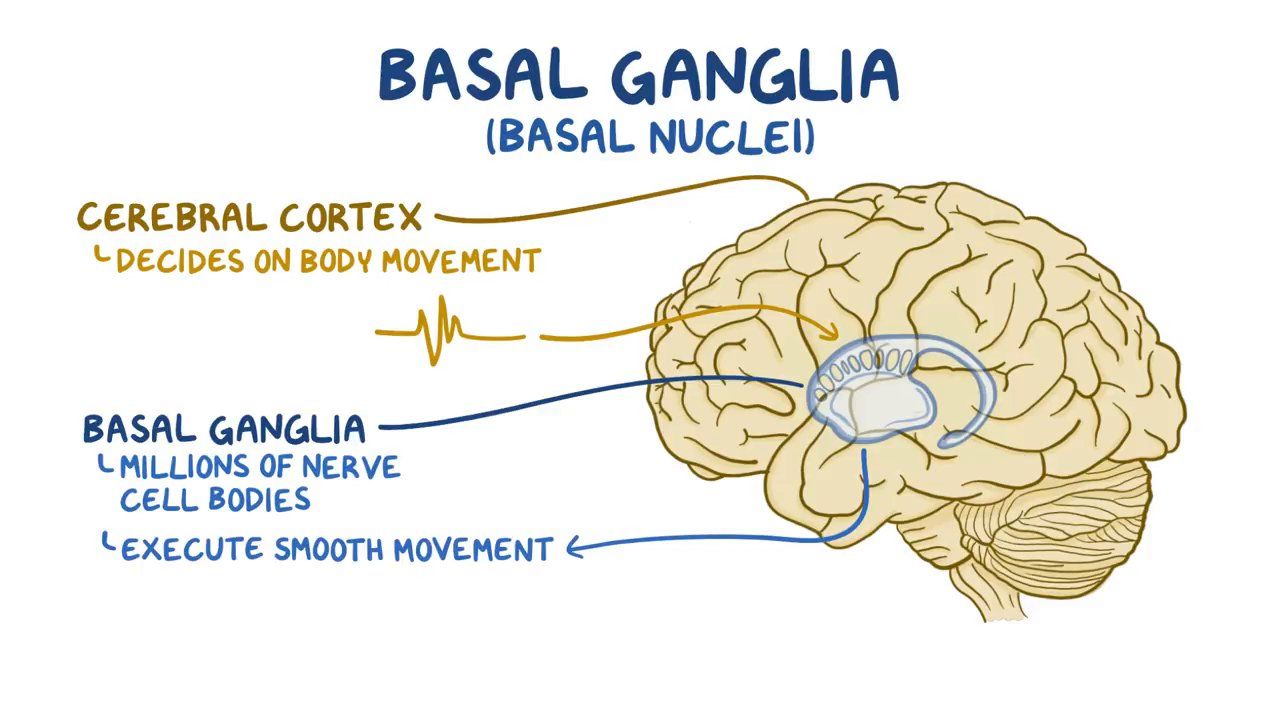
The basal ganglia are one of the components in the neural chain that controls the voluntary motor activity. The basal ganglia consist of five pairs of nuclei: caudate nucleus, putamen, globus pallidus, subthalamic nucleus, and substantia nigra. The function of the basal ganglia is to fine-tune the voluntary movements. They do so by receiving the impulses for the upcoming movement from the cerebral cortex, which they process and adjust. They convey their instructions to the thalamus, which then relays this information back to the cortex. Basal ganglia mediate some and other higher cortical functions as well, such as planning and modulation of movement, memory, eye movements, reward processing, and motivation.
Certain movement disorders can be traced to pathologies in the basal nuclei, the most notable being Parkinson disease, which is related to deficiencies of dopaminergic cells of the substantia nigra.
Reticular Formation (RF) 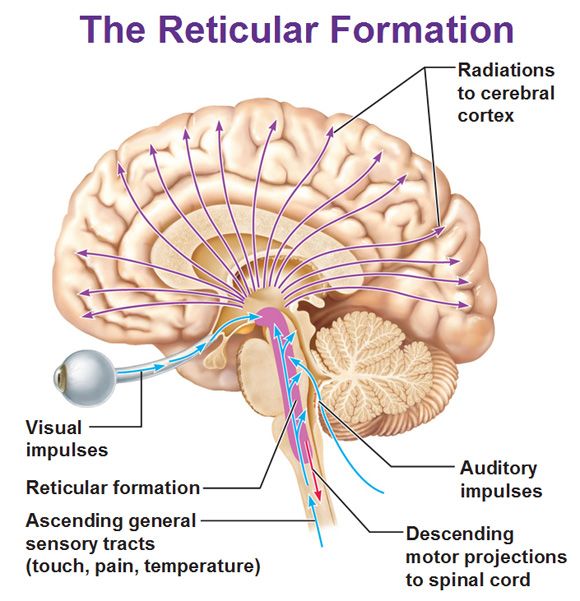
style=”color: #000000; font-size: 12pt;”>The reticular formation is a netlike structure of cells and fibres that extends throughout the core of the brainstem. It has a far-reaching network of neurons extending from the spinal cord to the thalamus, with connections to the medulla oblongata, midbrain, pons, and diencephalon. The RF plays a major integration and relay center for many vital brain systems to coordinate functions necessary for survival. It works together with other regions of the central nervous system to allow regulation of our state of consciousness, emotion processing, visual coordination, cardiovascular control, and posture.
The RF has two systems, an ascending and a descending:
The Ascending Reticular Activating System (ARAS) brings sensory messages from the RF to the brain cortex and vice versa. The ARAS is the regulator of consciousness and arousal and other information e.g. respiration rate, cough response, cardiac rhythm, and mastication (chewing).
The Descending Reticular System (DRS) brings messages to and from the motor neurons of the spinal cord. The reticulospinal tracts are the major descending pathways from the reticular formation and act on many levels of the spinal cord to coordinate movements and autonomic functions. They help to modulate tone, balance, posture, and coordination of body movements with the assistance of other sensory stimuli, such as visual, auditory, vestibular, and proprioceptive information.
Extensive damage to the reticular formation is incompatible with survival.
BRAINSTEM
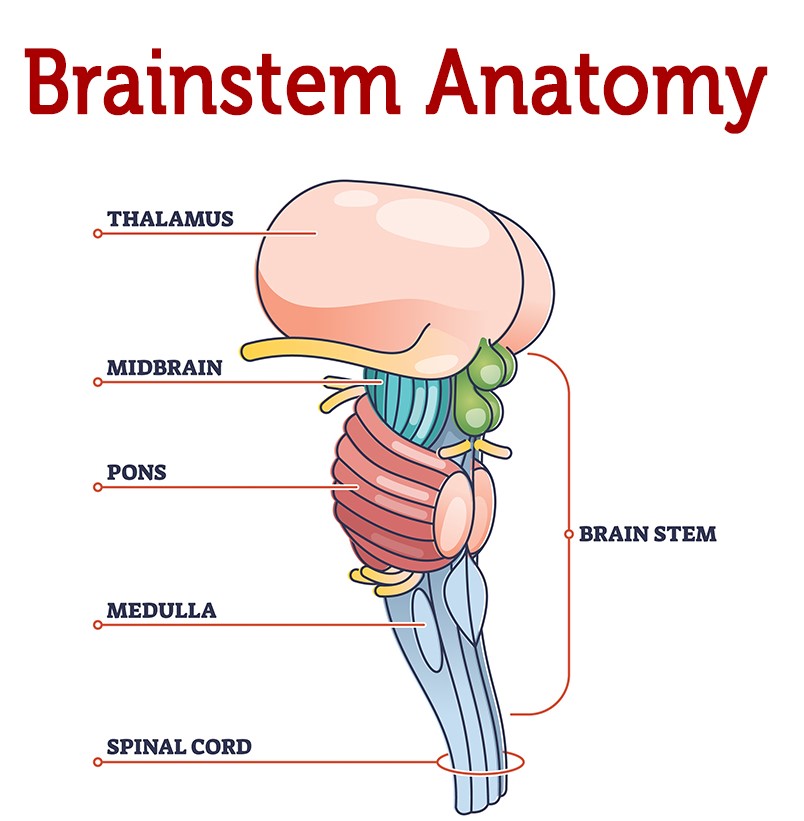
The brainstem consists of three parts: midbrain, pons and medulla oblongata.
It has three main important functions:
a. It contains the nuclei of the majority of the cranial nerves.
b. Facilitates the trajectory of neural pathways traveling between the spinal cord and brain.
c. Regulates vegetative functions such as heart rate, blood pressure, breathing and gastrointestinal functions.
Midbrain
The midbrain is involved in visual and auditory reflexes, alertness and temperature control. The midbrain contains the oculomotor nerve (CN III) and the trochlear nerve (CN IV).
Pons
The pons is involved in various functions like sleep, hearing, swallowing, taste, respiration, equilibrium and motor actions. Four pairs of cranial nerves emerge from the pons: trigeminal (CN V), abducens (CN VI), facial (CN VII) and vestibulocochlear (CN VIII) nerves.
Medulla oblongata
The medulla oblongata regulates autonomic activities related to cardiac, respiratory, reflex, and vasomotor functions. Within the medulla are several regions of gray matter that process involuntary body functions related to homeostasis. The cardiovascular center of the medulla monitors blood pressure and oxygen levels and regulates heart rate to provide sufficient oxygen supplies to the body’s tissues. The medullary rhythmicity center controls the rate of breathing to provide oxygen to the body. Vomiting, sneezing, coughing, and swallowing reflexes are coordinated in this region of the brain as well. Hypoglossal (CN XII), Glossopharyngeal (CN IX) and Vagus nerves (CN X) emerge from here.
CEREBELLUM
The cerebellum helps to control motor functions such as balance, posture, and coordination of complex muscle activities. The cerebellum receives sensory inputs from the muscles and joints of the body and uses this information to keep the body balanced and to maintain posture. The cerebellum also controls the timing and finesse of complex motor actions such as walking, writing, and speech. In adjusting and fine-tuning motor programs to make precise movements in a trial-and-error process, the cerebellum plays a major role in motor learning.
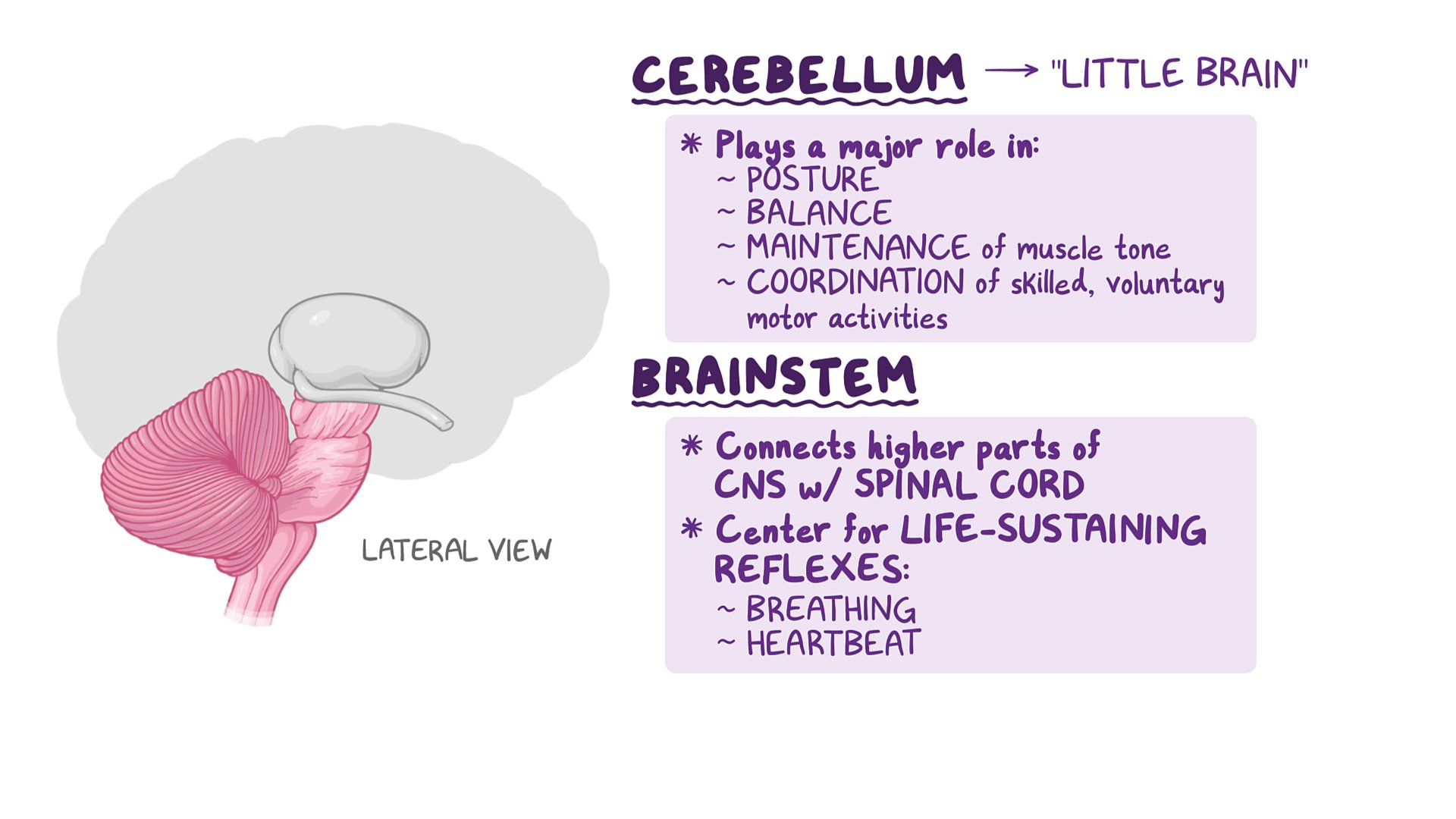
Cerebellar damage produces disorders in fine movement, equilibrium, posture, and motor learning depending on the part of the cerebellum involved and how it is damaged. Dysfunction may result in; Hypotonia (reduced muscle tone), Ataxia, Dysarthria (the inability to articulate words properly), Nystagmus (rapid jerky eye movements).
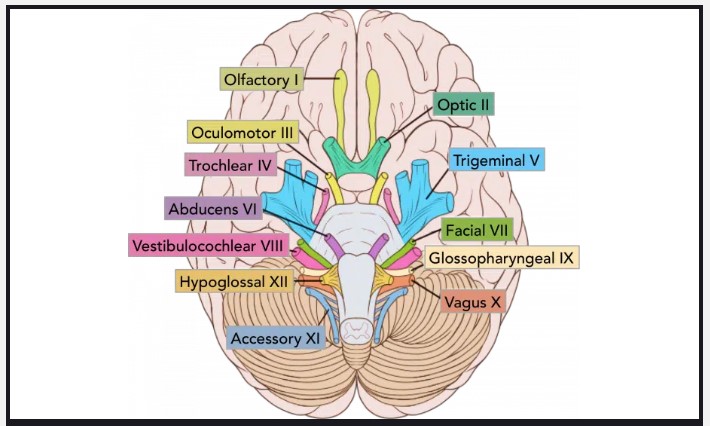 CRANIAL NERVES
CRANIAL NERVES
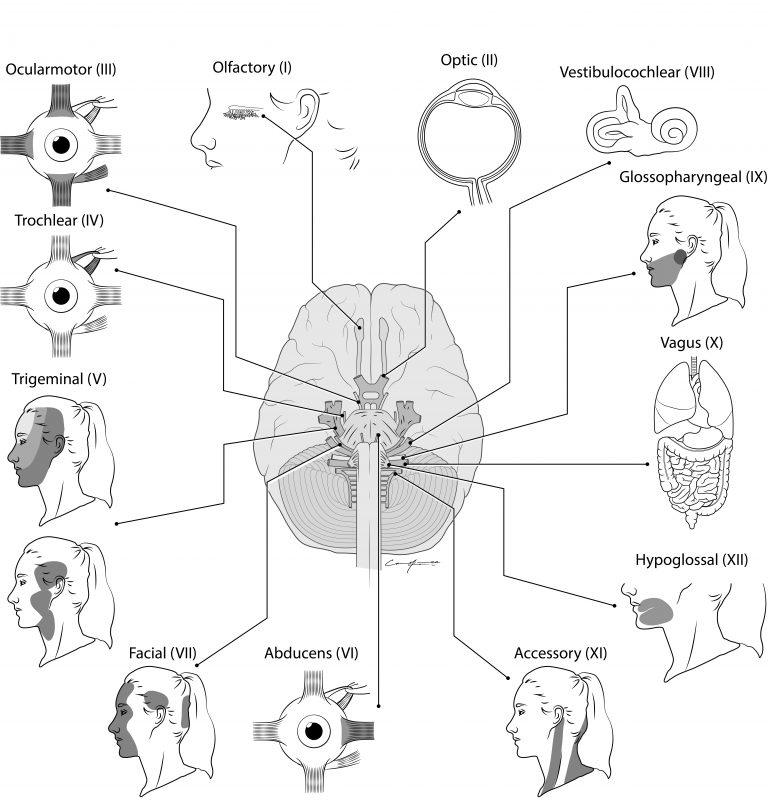
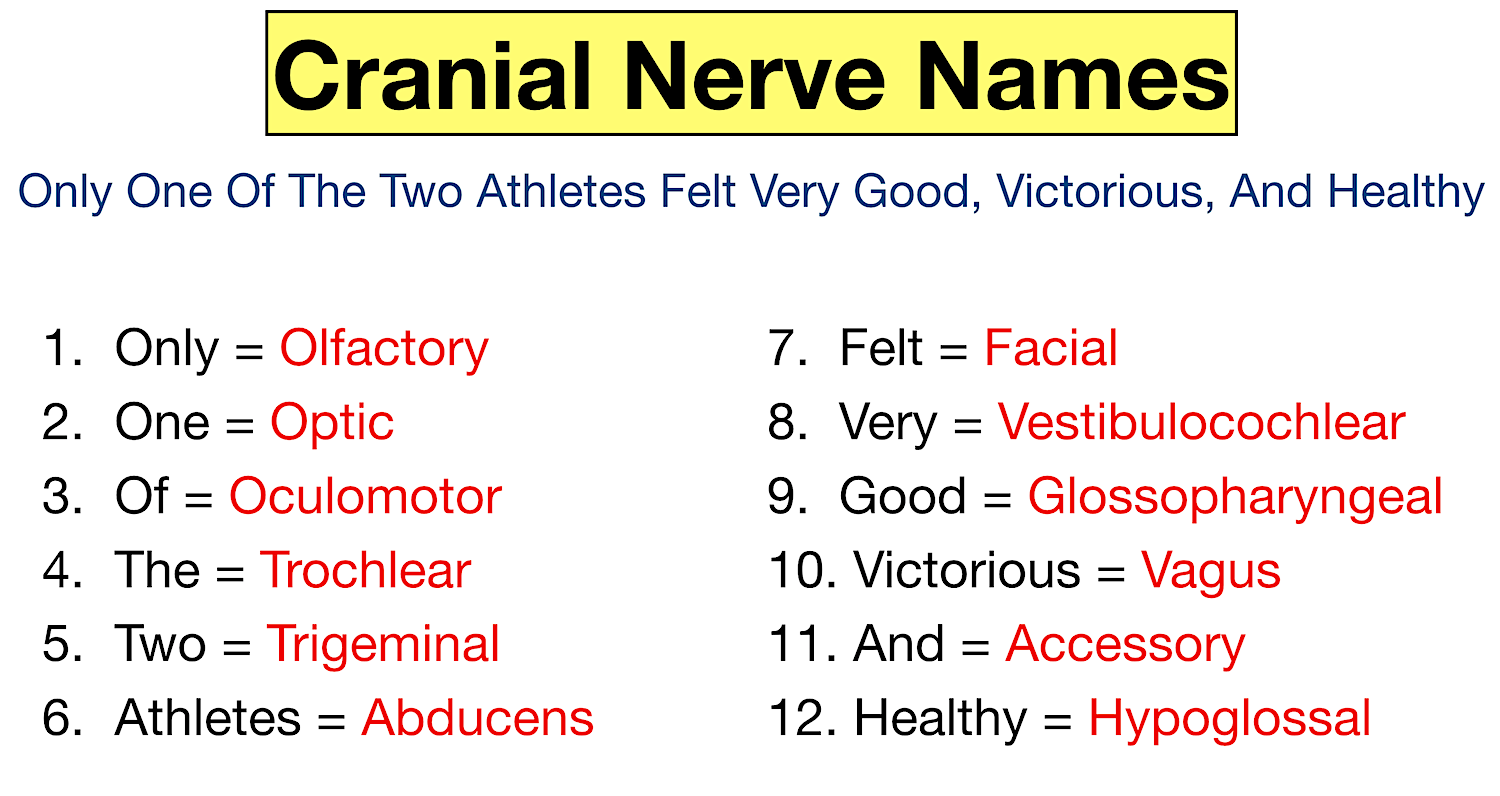
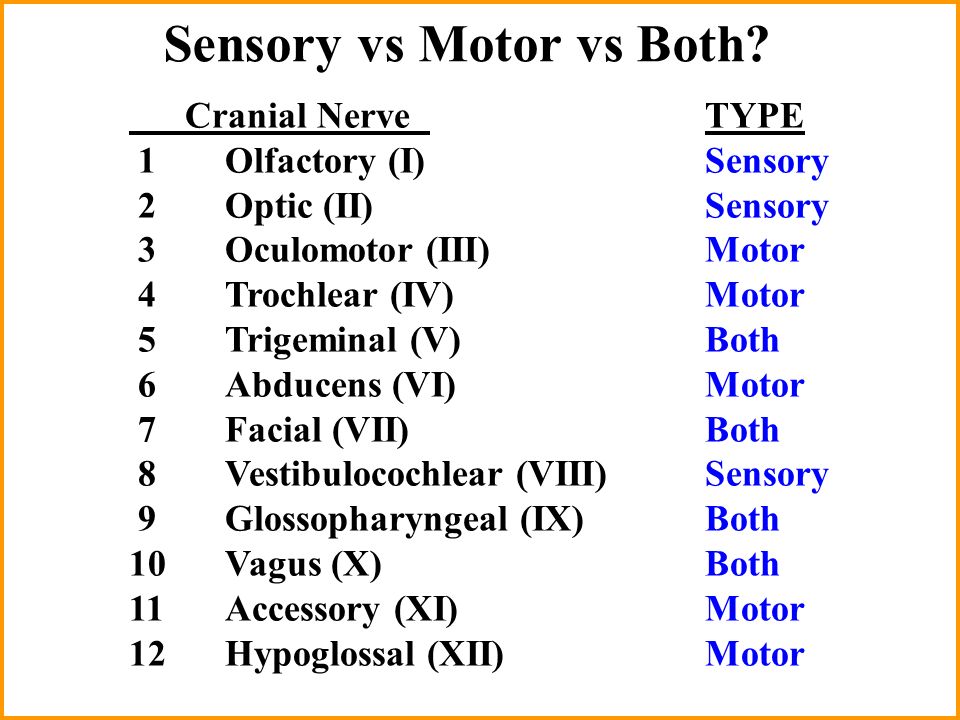
The cranial nerves are a set of 12 paired nerves that arise directly from the brain. The names of the cranial nerves relate to their function and they are numerically identified in roman numerals (I-XII).
. . .
Cranial nerves may contain motor, sensory or both types of fibres. They supply sensory and motor information to structures of the head and neck, controlling the activity of this region. Only the vagus nerve extends beyond the neck, to innervate thoracic and abdominal viscera.
.. ……………… 
| NAME | TYPE OF NERVE | FUNCTION | ASSESSMENT | |
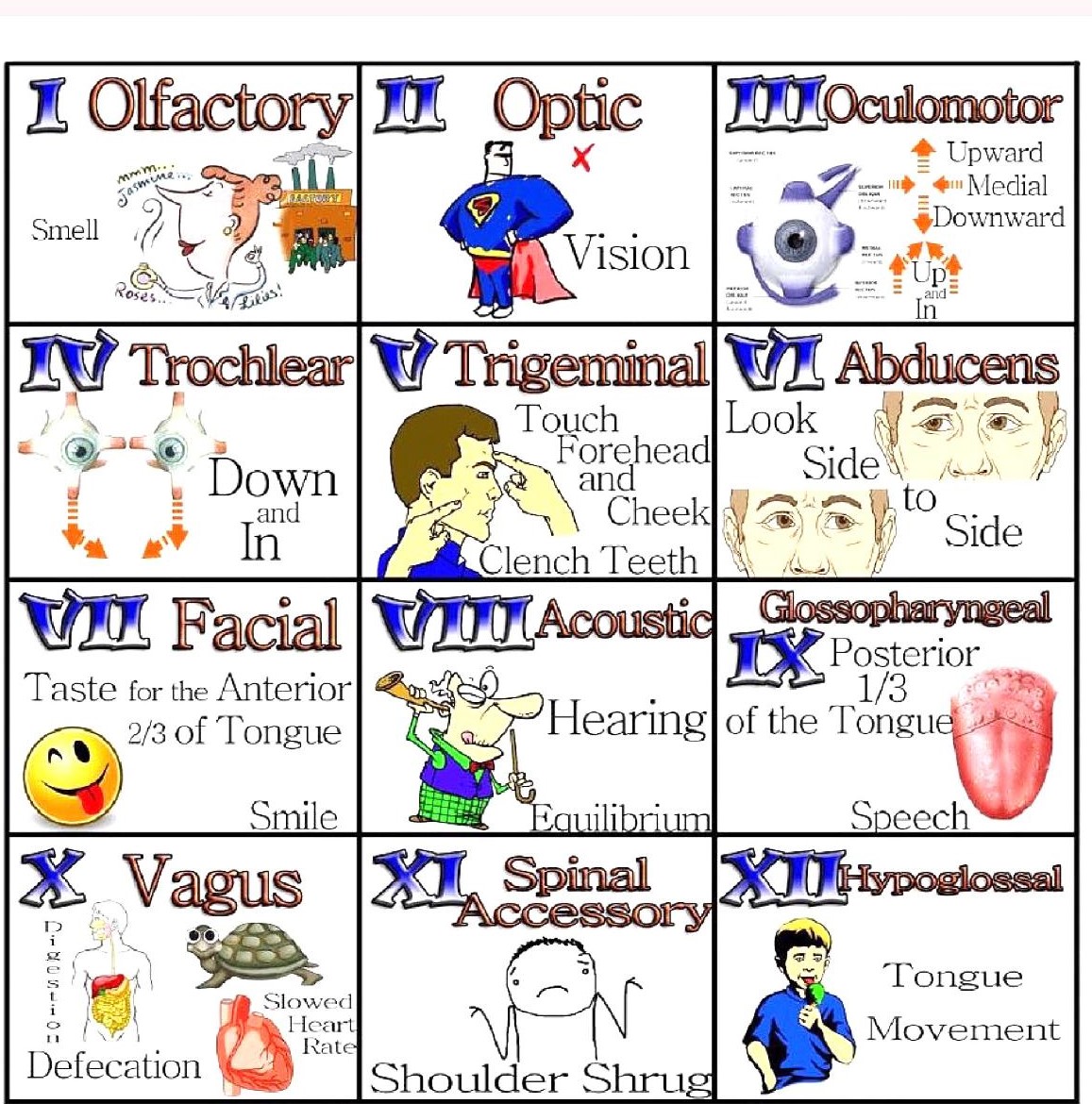
| Cranial Nerve 1 (CN I) | Olfactory nerve | Sensory | Smell | The patient is asked to identify odors (eg, soap, coffee, cloves) presented to each nostril while the other nostril is occluded |
| Cranial Nerve 2 (CN II) | Optic nerve | Sensory | Vision | Visual acuity is tested using a Snellen chart for distance vision or a handheld chart for near vision. Each eye is assessed individually, with the other eye covered. |
| Cranial Nerve 3 (CN III) | Oculomotor nerve | Motor | The oculomotor (CN III), trochlear (CN IV) and abducens (CN VI) nerves transmit motor information to the extraocular muscles to control eye movement and eyelid function. The oculomotor nerve also carries parasympathetic fibres responsible for pupillary constriction.
– Most eye movements |
Because the oculomotor, trochlear, and abducens nerves control related functions of the eye, they are tested as a unit. |
| Cranial Nerve 4 (CN IV) | Trochlear nerve | Motor | Eye movements | Tested as a unit. CN III: Oculomotor, CN IV Trochlear, CN VI Abducens |
| Cranial Nerve 5 (CN V) | Trigeminal nerve | Mixed | Motor: Muscles of mastication (chewing)
Sensory: Facial sensation |
Motor: motor function is tested by palpating the masseter muscles while the patient clenches the teeth and by asking the patient to open the mouth against resistance. If a pterygoid muscle is weak, the jaw deviates to that side when the mouth is opened.
Sensory: facial sensation (pin prick & light touch) |
| Cranial Nerve 6 (CN VI ) | Abducens nerve | Motor | Eye movements – Look laterally |
Tested as a unit. CN III: Oculomotor, CN IV Trochlear, CN VI Abducens |
| Cranial Nerve 7 (CN VII) | Facial nerve | Mixed | Motor: Facial expression, tearing and salivation
Sensory: Taste from the anterior two-thirds of the tongue. |
Motor: Check for hemifacial weakness.. Test motor function of the facial muscles and look for asymmetry: raise eyebrows, frown, smile, close eyes tightly, puff cheeks, etc.
Sensory: Taste in the anterior two thirds of the tongue can be tested with sweet, sour, salty, and bitter solutions applied with a cotton swab first on one side of the tongue, then on the other. Disease of the facial nerve results in peripheral facial paralysis (Bell’s palsy) on the side of the lesion. Causes of Bell’s palsy include compression of the nerve by a tumor and infections that inflame the nerve and surrounding tissue. The affected individual will be unable to close the eye on that side, wrinkle his or her forehead, or show teeth. Loss of muscle tone on the side of the lesion causes the corner of the mouth to droop. |
| Cranial Nerve 8 (CN VIIII) | Vestibulocochlear nerve | Sensory | Auditory and vestibular input – Sense of hearing and balance. |
Hearing tests- Hearing is first tested in each ear by whispering something while occluding the opposite ear. Any suspected loss should prompt formal audiologic testing to confirm findings and help differentiate conductive hearing loss from sensorineural hearing loss. Vestibular function tests- Vestibular function can be evaluated by testing for nystagmus. |
| Cranial Nerve 9 (CN IX) | Glossopharyngeal nerve | Mixed | Motor: Swallowing and speech.
The glossopharyngeal nerve transmits motor information to the stylopharyngeus muscle which elevates the pharynx during swallowing and speech. Sensory: Taste from the posterior third of the tongue. |
Usually assessed with CN X
Ask the patient if they have experienced any issues with swallowing, as well as any changes to their voice or cough. |
| Cranial Nerve 10 (CN X) | Vagus nerve
The vagus nerve serves as the body’s superhighway, carrying information between the brain and the internal organs and controlling the body’s response in times of rest and relaxation. The vagus nerve is the longest mixed cranial nerve. In detail: Motor: |
Mixed |
Motor: Transmits motor information to several muscles of the mouth which are involved in the production of speech. Gag reflex. Sensory: Conveys visceral sensation to the brainstem and also controls some visceral functions, such as heart rate and gastrointestinal motility |
Usually assessed with CN IX |
| Cranial Nerve 11 (CN XI) | Accessory nerve (Spinal Accessory) | Motor | Shoulder and neck muscle movement. | Evaluated by testing the muscles it supplies: • For the sternocleidomastoid, the patient is asked to turn the head against resistance supplied by the examiner’s hand while the examiner palpates the active muscle (opposite the turned head). • For the upper trapezius, the patient is asked to elevate the shoulders against resistance supplied by the examiner. |
| Cranial Nerve 12 (CN XII) | Hypoglossal nerve | Motor | Tongue movements | Ask the patient to extend the tongue and move from side to side while inspecting it for atrophy, fasciculations, and weakness (deviation is toward the side of a lesion). |
Assessment of CN III, IV, and VI: Oculomotor, Trochlear, and Abducens Nerves
Because the oculomotor, trochlear, and abducens nerves control related functions of the eye, they are tested as a unit.
Six extrinsic muscles move the eyeball within the orbit. The inferior, superior, and medial recti muscles and the inferior oblique muscle are controlled by the oculomotor nerve. The lateral rectus is controlled by the abducens nerve, and the superior oblique muscle is controlled by the trochlear nerve. For these cranial nerves, the patient’s eyes are observed for symmetry of movement, asymmetry or droop of the eyelids (ptosis), and twitches or flutters of eyes or lids. Extraocular movements controlled by these nerves are tested by asking the patient to follow a moving target (eg, examiner’s finger, penlight) to all 4 quadrants (including across the midline) and toward the tip of the nose; this test can detect nystagmus and palsies of ocular muscles. The pupillary light response is tested for symmetry and briskness. Anisocoria or differences in pupillary size should be noted in a dimly lit room.
Assessment of CN IX and CN X nerves which can be assessed together
A common test to determine IX and X function is to ask a patient to open his or her mouth and say “ahh.” The position of the soft palate and uvula at rest and with phonation is noted. Normally, the uvula and palate rise in the midline with phonation. Paralysis of cranial nerves IX or X on one side of the brain will cause the palate and uvula to deviate to the un-paralyzed side during phonation.
• Let the patient say “ah” and observe the soft palate elevating and that the uvula remain in midline
• Listen to voice quality
• Test for difficulty swallowing- Ask the patient to take a small sip of water (approximately 3 teaspoons) and observe the patient swallow. The presence of a cough or a change to the quality of their voice suggests an ineffective swallow which can be caused by both glossopharyngeal (afferent) and vagus (efferent) nerve pathology.
 ..
.. 
BLOOD SUPPLY
An adequate supply of oxygen and nutrients is vital for the normal function of the brain, which is achieved through a dense network of blood vessels. Arterial blood supply to the brain comes from four vessels, the right and left Internal Carotid and the right and left Vertebral Arteries, which join at the base of the brain to form the basilar artery.
Internal Carotid Arteries
The internal carotid artery on each side terminates into the anterior cerebral artery, the middle cerebral artery, and the posterior communicating artery.
Vertebral Arteries
On its journey to becoming the basilar artery, the vertebral arteries give off a number of branches, including the posterior spinal artery, posterior inferior cerebral artery and the anterior spinal artery. These constitute the blood supply to the upper cervical cord. The posterior inferior cerebral artery supplies the lateral medulla and cerebellum. Damage to these blood vessels can result in motor loss or sensory loss.
Basilar Artery
Formed by the two vertebral arteries. This has a number of branches: anterior and inferior cerebellar artery, artery to the labyrinth, pontine branches and superior cerebellar artery which supply the brain stem and cerebellum.
Anterior Cerebral Arteries
The anterior cerebral artery arises from the internal carotid. They are one of a pair of arteries that supplies oxygenated blood to most midline portions of the frontal lobes and superior medial parietal lobes.
Middle Cerebral Arteries
These supply parts of the frontal, temporal, occipital and parietal lobes bilaterally, with branches also supplying the basal ganglia and posterior limb of the internal capsule.
Posterior Cerebral Arteries
These supply blood to the posterior parietal cortex, occipital lobe and inferior temporal lobe. There are several branches of this artery that supply the midbrain, thalamus, subthalamus, posterior internal capsule, optic radiation and cerebral peduncle.
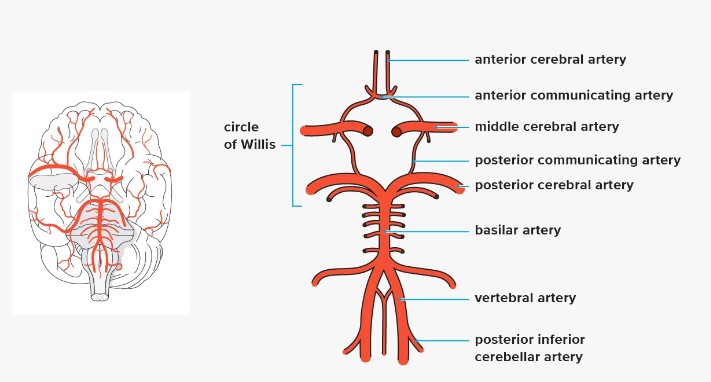
Circle of Willis
The basilar artery, the posterior cerebral arteries, the posterior communicating arteries, and the anterior cerebral arteries, along with the anterior communication artery, form an important collateral circulation, the Anterior and Posterior Circulation anastomose at the base of the brain, termed the Circle of Willis. These vessels lie within the subarachnoid space and are a common location for cerebral aneurysms to form.
References:
https://www.innerbody.com/image/nerv02.html
https://emedicine.medscape.com/article/1898830-overview?form=fpf#a2
https://www.kenhub.com/en/library/anatomy/the-central-nervous-system
https://www.physio-pedia.com/Brain_Anatomy
https://www.simplypsychology.org/limbic-system.html
Address : 11777 San Vicente Blvd, Los Angeles, CA 90049 suite # 502
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included

