


Allen Cognitive Levels
The Allen Cognitive Levels were developed by Claudia K. Allen, MA, OT, FAOTA, and colleagues in the late 1960s and 1970s to provide a classification system of function based on cognitive performance. The charts in this document will review the Allen Cognitive Levels, the Allen Cognitive Levels Screening Assessment (ACL), and examples of the application of the Allen Cognitive Levels to functional performance. The ACL levels are split up into sublevels, as identified by the Allen Cognitive Levels Screening Assessment (discussed in subsequent charts).
 The Allen Cognitive Level Screen (ACLS)
The Allen Cognitive Level Screen (ACLS)
The Allen Cognitive Level Screen (ACLS), also known as the leather lacing tool and the leather lacing test, is an evidence-based, standardized screening assessment of functional cognition. The ACLS gives you a quick measure of a person’s global cognitive processing capacities, learning potential, and problem-solving abilities during the performance of three visual motor tasks of increasing complexity.
The ACLS-5 Manual provides details for administering and scoring the test. The lacing tool used in this screening assessment is available in three forms:
1. Standard Allen Cognitive Level Screen (ACLS)
2. Large Allen Cognitive Level Screen (LACLS) for persons with vision or hand function problems
3. Disposable Large Allen Cognitive Level Screen (LACLS (D)) for single or serial use with individuals for whom infection control precautions must be observed.
To administer the ACL, the OT practitioner presents the individual with 3 visual-motor tasks of increasing complexity.
3 Visual-Motor Tasks = 3 Types of Stitches:
1. Running Stitch
• Allows the OT practitioner to judge the individual’s abilities for completing BADLs.
• Can help coach caregivers on what supports to provide.
2. Whip Stitch
• Allows the OT practitioner to judge the individual’s problem-solving abilities.
• Can help determine whether they can prepare a meal, remember to take their medications, respond to emergency situations like a smoke detector going off.
3. Cordovan Stitch
• Allows the OT practitioner to judge the individual’s ability to processes information.
• Can help determine whether they can hold a job, drive, or take care of others.
For more information on the ACLS please refer to the following links:
https://allencognitive.com/
https://allencognitive.com/acls-5-lacls-5/assessments-1-acls_lacls/
https://allencognitive.com/free-offerings/
https://www.crisisprevention.com/Blog/Cognitive-Assessment-Tools
Allen Cognitive Levels

An easy mnemonic to help you remember the different levels:
“All players must get extra points”
1. Automatic
2. Postural
3. Manual
4. Goal directed
5. Exploratory
6. Purposeful
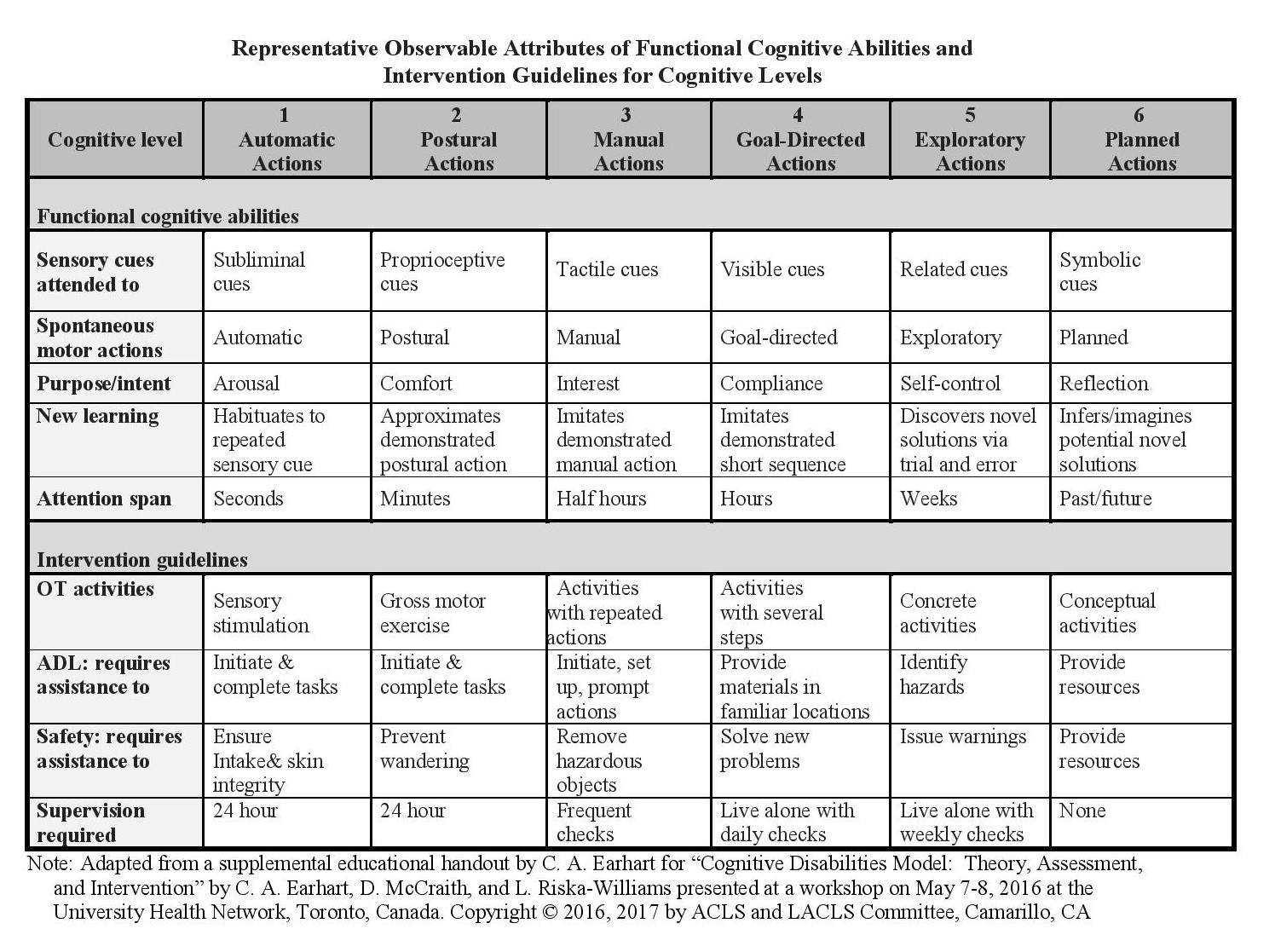
OVERVIEW OF ALLEN COGNITIVE LEVELS
– Presented in 6 Charts
CHART 1.
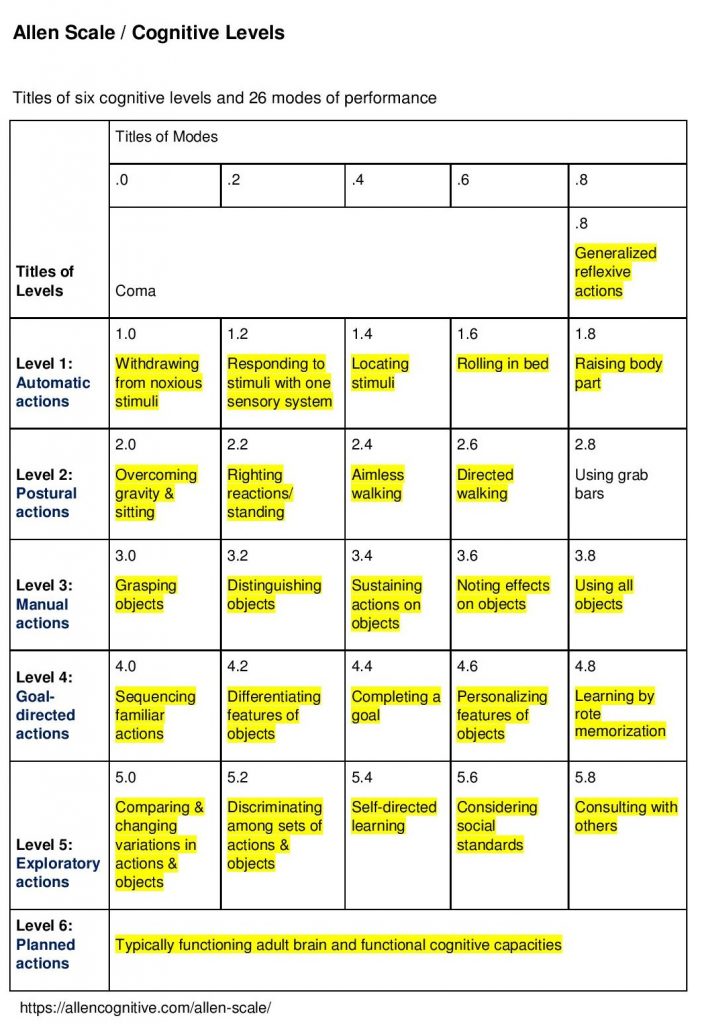
CHART 2.
| Summary of ACL Levels |
| Level 1 describes automatic actions (e.g., swallowing, diverting attention towards stimuli). In other words, Level 1 describes the patient’s arousal to external cues. This cognitive level is largely instinctual behavior, and patients require total assistance with activities. A patient who is below cognitive level 1 would be in a coma. |
| Level 2 describes postural actions (e.g., gross movement in response to proprioceptive cues). The motivation for the patient’s actions is primarily comfort or discomfort, remaining mostly unaware of the effects of their actions on their surroundings. Aimless pacing and/or wandering are observable in patients functioning at this cognitive level. Patients at Level 2 require maximum assistance. |
| Level 3 describes manual actions (e.g., grasping at and using objects). What distinguishes Level 3 from Level 2 is the increased ability to discriminate the external from the self. The patient’s global cognition remains impaired at this level, but long-term repetitive training can allow these patients to acquire new behaviors by better noting their effects on objects, sustaining their actions, and utilizing materials for ADLs. Despite their ability to sustain actions, patients at Level 3 still lack sustained concentration and may need frequent re-direction to complete tasks appropriately; moderate assistance is a recommendation for Level 3. 24-hour supervision should be in place for patients at Levels 1, 2, and 3. |
| Level 4 describes goal-directed actions (e.g., preparing a snack, following a route around a familiar neighborhood). At this level, the patients can recognize and understand the effect their actions have on their surroundings. Relying on visible cues, they can learn and carry out activities specific to particular goals. However, patients functioning at Level 4 still have trouble recognizing finer details and learning independently. Hence, they often lack the cognitive skills to identify and fix errors, and supervision in the form of minimum assistance is the recommendation for these patients. |
| Level 5 describes exploratory actions (e.g., problem-solving through trial-and-error). Patients at Level 5 of the ACLs can learn by emulation of actions shown to them. They are also able to apply what they learn to other activities and situations. Still, these patients have limited ability to organize, anticipate, and plan. This limitation can lead to poor judgment and higher impulsivity, especially in situations that require more deductive reasoning. External cues via supervision can help patients at this cognitive level plan. Patients at Level 5 should receive standby assistance. |
| Level 6 describes planned actions (e.g., anticipation and prevention of errors). There is no global cognitive impairment at this level, and the patient at this ACL is considered to be a normally functioning adult. It is important to note that because the ACLs describe cognitive levels, the patient may still have physical limitations. There is no supervision required at Level 6. |
https://www.ncbi.nlm.nih.gov/books/NBK556125/
CHART 3.
| Level | Name | Characteristics | Intervention | Video Example |
| Level 1 | Automatic Actions |
Global cognition is profoundly impaired -Automatic motor responses. Behavior is mostly reflexive |
Sensory Stimulation * Total care 24 hours a day is necessary 1.0: Withdrawing from Noxious Stimuli |
An occupational therapy student explains the Allen Cognitive Levels using stick figure illustrations. |
| Level 2 | Postural Actions |
Global cognition is severely impaired -Can be stimulated to perform postural actions in response to proprioceptive cues ACLS – Unable to imitate the running stitch |
Movement or exercise groups based on imitation * 24 hour close on-site supervision required
* Safety risk for wandering 2.0 Overcoming Gravity |
An occupational therapist explains the Allen Cognitive Levels using a whiteboard chart. |
| Level 3 | Manual Actions, depends on interest in objects at arm’s reach |
Global cognition is severely impaired –Uses hands to manipulate objects |
Repetitive tasks including ADLs * Need for supervision and assistance with ADLs |
An occupational therapist administers the ACLS to a nursing home resident with dementia. |
| Level 4 | Goal Directed Actions |
Global cognition is moderately impaired * Big step for independence -Activities are purposeful and able to perform short tasks ACLS – Able to imitate the whip stitch, three stitches |
Reinforce familiar routines and perform repetitive drilling * Requires 24-hour supervision to maintain safe surroundings, support consistent routines and assist with solving problems as they arise 4.0 Sequencing |
Occupational therapy students demonstrate Allen Cognitive Level 4. |
| Level 5 | Exploratory Actions |
Global cognition is mildly impaired -New learning can occur ACLS – Able to imitate the single cordovan stitch using overt trial and error methods, three stitches |
Standby Assistance 5.0 Continuous Neuromuscular Adjustments |
An occupational therapist administers the ACLS to a nursing home resident with multiple health problems. |
| Level 6 | Planned Actions |
No global cognitive impairment * Typically functioning adult brain and functional cognitive capacities |
No supervision required. * Therapist serves as a collaborative consultant in the treatment process, providing new information to adjust to a physical disability 6.0 Planning without Objects |
Occupational therapy students demonstrate Allen Cognitive Level 5. |
CHART 4.
| Level | Cognition | FIM | Level of Assist | Attention Span | Manual Activities |
| 1 | Global cognition is profoundly impaired.
Responds to internal cues only. |
Level 1
Complete dependence |
Total Assistance | Seconds | No level of participation in any manual activity.
Motor actions are Automatic/Reflexive. |
| 2 | Global cognition is severely impaired.
Awareness is limited to own postural actions (proprioceptive cues) to move body in space or overcome effects of gravity. |
Level 2
Complete dependence |
Max Assistance | Minutes | No level of participation in any manual activity.
|
| 3 | Global cognition is severely impaired.
Performs spontaneous manual actions in response to tactile cues. Repetitive actions, demonstrates an awareness of material objects but lack of awareness of end product/goal. |
Level 3
Modified dependence |
Mod Assistance | 30 minutes | Simple manual tasks with repetitive and routine steps.
3.0 Grasp objects – purposeful grasp and release 3.2 Distinguishes between objects 3.4 Sustains actions on objects (may look perseverative) 3.6 Cause and effect – notices effects have on objects, by manipulating them e.g. able to sort objects, uses mirrors during ADLs 3.8 Uses all objects and knows when an activity is completed |
| 4 | Global cognition is moderately impaired.
Aware of tangible cues (what can be seen and touched) and understands visible cause-and-effect relationships. Goal-directed actions, demonstrates an awareness of a familiar end-product but fails to solve new problems, anticipate, or correct mistakes. There is no independent new learning and cannot invent new motor actions. |
Level 4
Modified dependence |
Min Assistance | Hour
Attention span is usually good for up to one hour. |
Goal-directed motor actions. |
| 5 | Global cognition is mildly impaired.
Able to learn new ways of doing things through trial-and-error problem solving. Detects the best effect by exploring distinctive properties of objects and trying different actions. Poor judgment with no symbolic thought to plan actions or anticipate potential mistakes. Make hasty or impulsive decisions or make abrupt changes in course of action. The determination of what is best may be made according to personal preferences or social standards. Can imitate a series of new directions; new learning is recognized and repeated during the process of doing an activity. |
Level 5
Supervision Distant supervision with weekly visits and verbal cuing (checking the safety, giving advice) |
Standby Assistance | Weeks | Able to imitate a series of new directions; new learning is recognized and repeated during the process of doing an activity. |
| 6 | Absence of cognitive disability
Absence of dysfunction, task performance is planned and premeditated, anticipates errors, and able to use abstract and symbolic reasoning. Considers several hypothetical plans of actions and establishes abstract criteria for selecting the best plan. Able to make plans for the future, taking into account possible risks to health and well-being for one’s self and others. |
Level 6-7
Modified- Complete independence |
Independent | Attention span is defined by desires and priorities | Absence of dysfunction. |
FIM LEVELS
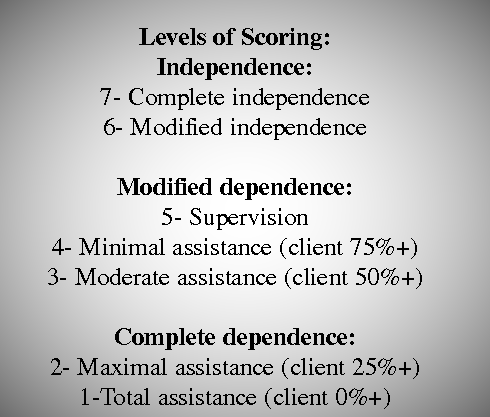
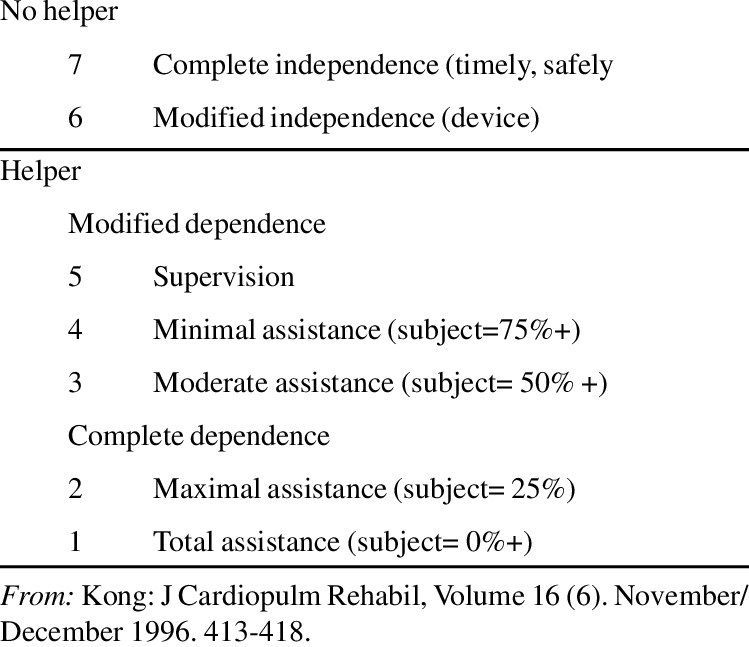
CHART 5.
| Level | Accommodation | Abilities | Employment | Picture |
| 1 | Requires 24-hour total nursing care. | May tolerate hand-over-hand oral feeding techniques. |  |
|
| 2 | Requires 24-hour assistance to initiate and assist with daily activities of daily living | Level 2.0 – assists with transfers and body position changes.
Level 2.4 – gross body movements, aimless walking. Level 2.8 – may use grab bars and furniture to stabilize their balance. |
 |
|
| 3 | Group home – 24-hour supervision. | With assistance and supervision, able to perform BADLs. | Supported employment. Unskilled work in sheltered workshop, with supervision. |  |
| 4 | Level 4.4 – May live with someone who does a daily check on the environment and removes any safety hazards and solves any new problems. May be left alone for part of the day with procedure for obtaining help by phone or from a neighbor.
Level 4.6 – May live alone with daily assistance to monitor personal safety. May require reminders to do household chores. Level 4.8 – May live alone with daily assistance to monitor safety and check problem- solving methods.
|
Level 4.0 – May fix self a cold meal or snack and make small purchases in the neighborhood.
Level 4.2 – May spend a daily allowance, walk to familiar locations in the neighborhood, or follow a simple, familiar bus route. Level 4.4 – May manage a daily allowance and go to familiar places in the neighborhood. Level 4.6 – May require reminders to attend familiar community events, or to do anything in addition to daily household routine. Level 4.8 – May get self to a regularly scheduled community activity.
|
Level 4.8 – may succeed in a supportive employment environment. |
|
| 5 | Level 5.0 – May live alone with weekly checks to monitor safety and check problem-solving methods.
Level 5.2 – May live alone with weekly checks to monitor safety and examine potentially dangerous effects of impulsive behavior. Level 5.4 – May live alone.
|
Level 5.6 – May drive. | Level 5.0 and 5.2 – May succeed in supportive employment with a job coach.
Level 5.4 – May work in a job with a wide margin of error. May not be safe in jobs with a high potential for industrial accidents. Level 5.6 – May work in a suitable job and be relied upon to consistently follow safety precautions.
|

|
| 6 | Independent | Independent | May work in competitive employment. |  |



CHART 6.
Use of the Allen Cognitive Levels
The Allen Cognitive Levels are designed to be used with any patient population that experiences temporary or permanent cognitive impairments. Following is a list of diagnoses that may be appropriate for the application of the Allen Cognitive Levels (not inclusive) and the ways the levels might be applied during occupational therapy treatment:
| Diagnosis | Implications for Occupational Therapy Treatment: the Allen Cognitive Levels can be used to: | Example |
| Alzheimer’s disease and senile dementia | 1. Determine current level of cognitive function and monitor decline in function. 2. Determine potential to live independently. 3. Determine level of skilled care required when no longer able to live independently. 4. Determine adaptations needed to participate in functional tasks. 5. Recommend adaptations and precautions for safety. |
A woman with advancing Alzheimer’s disease has been admitted to a nursing home by her family, who can no longer care for her. The occupational therapist administers the ACLS and determines that the woman is functioning at a Level 3.0. Based on this result, the occupational therapist recommends a bed alarm and wonder guard to help prevent the woman from falling or wandering out of the building unsupervised. |
| Cerebrovascular accident (CVA) | 1. Determine current cognitive function as compared to family report of function prior to CVA. 2. Track improvements in cognitive function as therapy progresses. 3. Help to make distinctions between cognitive impairments and expressive language limitations during functional tasks. 4. Contribute to the decision making process as the patient prepares to leave inpatient rehabilitation. |
An occupational therapist administers the ACLS to a man who has suffered a CVA when he is admitted to inpatient rehabilitation and determines that he is function at a level 4.2. She re-administers the ACLS two weeks later and the man obtains a score of 5.0. The occupational therapist recommends that the man be allowed to return to home but that his family should provide him with assistance with problem solving, decision making, and learning new activities. |
| Traumatic brain injury | 1. Determine current cognitive function as compared to family report of function prior to TBI. 2. Track improvements in cognitive function as therapy progresses. 3. Determine potential to return to home and work. 4. Determine the level of skilled care needed if unable to return to home. 5. Identify difficult behaviors that might interfere with the rehabilitation process. 6. Aid in referral to training programs and vocational rehabilitation. |
A young man who has sustained a traumatic brain injury in a car accident is referred to occupational therapy to assist in community placement following long term rehabilitation. The occupational therapist administers the ACLS and determines that the young man is functioning at a level 4.6. The occupational therapist recommends that the young man live in a supervised apartment setting with daily supervision and assistance with community mobility, banking, shopping, and other higher level tasks. |
| Developmental disability | 1. Identify cognitive function during daily activities. 2. Identify difficult behaviors that might interfere with intervention. 3. Develop training programs for pre-vocational and vocational skills. 4. Develop social skills programs. 5. Aid in supported employment and community placement. |
An occupational therapist administers the ACLS to a young adult woman who has just begun to attend a sheltered workshop. The therapist administers the ACLS and finds the woman is functioning at a level 3.4. The therapist recommends that the woman perform a single step job task using templates, with direct supervision. |
| Schizophrenia | 1. Determine changes in cognitive function due to relapse or medication changes. 2. Aid in the decision making process for community placement and vocational rehabilitation. 3. Identify difficult behaviors that might interfere with intervention. 4. Help to differentiate between cognitive function and symptoms of psychosis. |
A man with schizophrenia is ready to leave the inpatient psychiatric unit following a relapse. The occupational therapist administers the ACLS and determines that the man is functioning at a level 5.4. The occupational therapist recommends that the man return to his prior living situation, which was living independently in an apartment with weekly supervision from his family. |
| Bipolar disorder | 1. Determine changes in cognitive function due to relapse or medication changes. 2. Aid in the decision making process following relapse and inpatient hospitalizations. 3. Help to track the effectiveness of medications. 4. Determine functional abilities during community activities and vocational rehabilitation. |
A woman with bipolar disorder is admitted to the inpatient psychiatric unit during a severe depressive episode. The occupational therapist administers the ACLS and determines that the woman is functioning at a level 3.8. The occupational therapist informs the woman’s physician that the woman is not currently capable of living independently. |
| Chronic depression | 1. Help to identify long-term cognitive deficits vs. short term limitations due to acute or situational depression. 2. Help to track the effectiveness of medications. 3. Aid in decision making processes when depression occurs concurrent with physical disease or disability. 4. Aid in programming for community re-entry and vocational rehabilitation. |
An occupational therapist completes an evaluation with an outpatient referred for carpal tunnel syndrome, with a pre-existing diagnosis of chronic depression. The therapist determines that the patient’s cognitive level is 5.0. The therapist adapts her treatment plan to include adaptations for problem solving, decision making, and short term memory to help the woman comply with her carpal tunnel precautions. |
| Substance abuse | 1. Identify current cognitive function as compared to family report of prior cognitive function following overdose or inpatient admission for drug treatment. 2. Track improvements in cognitive function as therapy progresses. 3. Determine potential and level of support needed for community re-entry. 4. Aid in programming for outpatient support and vocational rehabilitation. |
A man with chronic alcoholism is admitted to the nursing home following guardianship proceedings. The occupational therapist administers the ACLS and determines that the man is functioning at a level 4.0. The occupational therapist uses the result to assist nursing and activities staff with program planning for the man. Her recommendations include monitoring of nutritional intake, set-up and stand-by supervision with self care tasks, and guided activities with staff or in groups. |
| Post-traumatic stress disorder and other anxiety disorders | 1. Help to differentiate between cognitive limitations prior to and following traumatic incidents. 2. Track improvements in cognitive function as therapy progresses. 3. Track changes in cognitive function due to medication and situational changes. 4. Aid in the decision making process regarding living situation and vocational rehabilitation. |
An occupational therapist completes an initial evaluation with a woman who has survived a house fire. The woman’s family reports she was completely independent with all tasks prior to the fire. The therapist administers the ACLS and determines that the woman is functioning at a level 5.0. The therapist determines that the trauma has affected the woman’s cognitive functioning and develops a treatment plan to address her cognitive deficits. |
| Post operative cognitive dysfunction | 1. Identify improvements in cognitive function as patients recover from surgery. 2. Determine ability to participate in inpatient rehabilitation and behaviors that might interfere with therapy. 3. Determine when patients have returned to prior levels of cognitive function. |
An occupational therapist completes an ACLS as a part of her initial evaluation with a man who has had open heart surgery and is displaying dementia. The man’s initial score on the ACLS is 3.2. The man’s family reports that he was independent with all activities prior to his surgery. The occupational therapist uses the ACLS to monitor the man’s cognitive level as he progresses through cardiac rehabilitation and identifies his cognitive level as a 5.6 when he is ready to leave the hospital. The therapist recommends that the man be discharged to home. |
References:
https://allen-cognitive-levels.com/allen-cognitive-levels-chart-and-description.html
https://allen-cognitive-levels.com/levels.htm
https://www.crisisprevention.com/Blog/October-2010/Middle-Stage-Dementia-Learning-to-Identify-Allen-L