
Splints

Splints are rigid or semi-rigid devices used to either support or immobilize an extremity.
There are two general purposes for the use of splints:
1. Splints are used to immobilize an extremity or part of an extremity during healing to prevent re-injury and promote correct alignment of the bones and tissues involved.
2. Splints are used to support an extremity or part of an extremity to align the extremity, allowing function.
Knowledge of splinting is necessary for occupational therapists who work with people with orthopedic and neurological conditions. The following charts will review the general considerations of splinting, as well as specific splints and their uses. A section on casting is also included.
General Considerations
When selecting a splint for a patient, the following points must be considered:
1. Diagnosis – what is the condition limiting the patient’s function?
2. Purpose – what is the overall purpose of the splint?
a. Immobilization for healing
b. Positioning for function
3. How will the splint be incorporated into the patient’s treatment plan?
a. Are there short or long-term goals addressing splint use?
b. Is there a plan to educate the patient on splint use?
4. Is the splint comfortable?
a. Are joints positioned correctly?
b. Have adjustments been made to avoid pressure areas?
c. Is padding positioned correctly?
5. How does the splint look? Will the patient accept and use the splint?
a. If the patient does not like the splint, he or she probably will not wear it.
Splinting Precautions
When fitting or fabricating a splint for a patient, the first precautions that must always be considered are those specified by the patient’s physician. If the patient is recovering from a specific surgery, such as a tendon graft or a complicated fracture, the physician will usually specify precautions to prevent injury to the surgical site. These precautions must be observed when splinting the surgical area.
If the physician has not provided specific precautions, then general splinting precautions may be observed as follows:
1. Make note of any pre-existing skin conditions or circulation problems.
a. Check for rashes and reactions to heat or splinting materials.
b. Take potential skin conditions into consideration if the patient has diabetes.
c. Consider edema and potential pressure areas if the patient has hemiparesis.
2. Adjust or fabricate splints to avoid bony prominences.
a. Splinting over bony prominences increases the chance for pressure sores to develop.
b. If a splint must cover a bony prominence, the area around the prominence should be padded and skin monitored.
3. Make sure the splint conforms to the area and fits snugly to avoid friction.
a. A poorly fitted splint may move and rub an area, creating sores and discomfort.
4. Monitor splints for pressure areas during use.
a. Limit the wearing time of a new splint to 1-2 hours at a time (unless otherwise ordered by the physician). Increase wearing time as the patient will tolerate.
b. Check for red areas when the splint is removed. If red areas persist or if cracking/bleeding appear, the splint must be adjusted.
Types of Splints
There are two general types of splints. Static splints do not have moving parts and position an extremity so that the splinted area is immobilized. These splints are usually fabricated out of low temperature thermoplastic, but may be made from a harder, less flexible material. Dynamic splints may have moving parts and position an extremity to facilitate movement. Dynamic splints may have thermoplastic bases combined with movable components, or may be made of softer materials such as neoprene or cloth. The following charts will review specific types of upper extremity static and dynamic splints.
Static Splints
| Splint Name | Description | Indications | Example | Photo |
| Resting pan splint | Provides support along the volar surface of the fingers, hand, wrist and forearm. The thumb is usually positioned in slight abduction. The splint may be padded for comfort.
A variation is the dorsal resting splint, where the wrist and forearm support is provided along the dorsal surface rather than the volar surface. The hand and finger pan still supports the volar surface. |
Used for conditions that require the hand and forearm to be immobilized for periods of time. -hemiparesis -arthritis -chronic pain conditions The dorsal resting pan splint is used when splint contact with the volar surface of the wrist and forearm is contraindicated. -skin conditions -IV or other ports -unable to fit a volar splint due to contractures or deformities | A man with left hemiparesis following a CVA wears a resting pan splint on his left hand to reduce edema and prevent contractures. |  |
| Anti-spasticity ball splint | Provides support along the volar surface of the fingers and hand. May also support the wrist and forearm. The fingers and thumb are spread into abduction by individual troughs. The name “ball splint” comes from the use of a ball to position the hand during manual fabrication of this splint. | Used to reduce spasticity and prevent contractures. -hemiparesis from CVA or TBI -cerebral palsy -multiple sclerosis and other degenerative neurological conditions -Alzheimer’s disease | A woman with cerebral palsy wears an anti-spasticity ball splint on her right hand at night to reduce muscle spasticity, keeping her hand open for functional use during the day. |  |
| Cone splint | This splint is shaped like a cone. The splint is placed in the hand with the narrow end toward the thumb and the wide end toward the little finger. A cone splint may be hand based or may be incorporated into a wrist/forearm splint with a trough along the ulnar side of the arm. | Used to position the hand when severe flexion contracture is already present. -hemiparesis -Alzheimer’s disease or dementia -advanced neurological conditions | A man with end stage Alzheimer’s disease wears cone splints on both hands to prevent skin breakdown and to allow some mobility for hygiene. |  |
| Wrist cock-up splint | Provides support to the volar surface of the wrist and forearm. The wrist is positioned in about 15 degrees of extension. A hole is incorporated into the splint to accommodate the thumb. May be made of thermoplastic or may be fabric with metal stays to immobilize the wrist. –A variation is the dorsal wrist cock-up splint, which provides support to the volar surface of the palm and the dorsal surface of the wrist and forearm. | Used for wrist injuries, median nerve compression injuries, and positioning when spasticity or deformity is present. -carpal tunnel syndrome -arthritis -simple wrist fractures -cerebral palsy | A secretary with carpal tunnel syndrome uses bilateral wrist cock-up splints to immobilize her wrists while typing. | Dorsal Volar   |
| Volar wrist splint | Similar in design to a wrist cock-up splint but the wrist is positioned in neutral. | Used for fractures, tenosynovitis, positioning after nerve injury or surgery for repetitive motion injuries. -carpal tunnel syndrome -wrist fractures -radial nerve palsy -rheumatoid arthritis | A woman wears a volar wrist splint on her left hand for 24 hours per day during the two weeks immediately following her carpal tunnel release surgery. |  |
| Thumb Spica splint (also called thumb opponens splint) | Provides support to the CMC and MCP joints of the thumb. May be hand based or may be incorporated into a wrist cock-up splint. May be made of thermoplastic or may be fabric with metal stays to immobilize the thumb. The thumb is positioned in opposition to the index finger. The PIP joint of the thumb is not immobilized to allow distal movement and opposition to the fingers. | Used for fractures, injuries, and repetitive motion syndromes of the thumb. -scaphoid, lunate, and first metacarpal fractures -de Quervain tenosynovitis (mommy thumb, gamer’s thumb) -damage to the ulnar collateral ligament -inflammation or deformity of the CMC or MCP joints due to arthritis or dislocation | A man with a diagnosis of de Quervain tenosynovitis wears a thumb spica splint to immobilize his thumb and relieve his symptoms while working at his job as a carpenter. | 
|
| Thumb extension splint | Positions the thumb in extension and prevents adduction and opposition. | Used to immobilize the thumb after tendon or ligament injuries. | A man wears a thumb extension splint to immobilize his thumb following repair of his abductor pollicis brevis tendon following a laceration injury. |  |
| C-bar splint | Positions the thumb in opposition to the index finger and maintains the web space between the thumb and index finger. This splint does not provide joint stabilization. | Used to prevent contracture following median nerve injuries. | A teenager with a partial median nerve laceration wears a c-bar splint to prevent his thumb from contracting into adduction while his injury heals. |  |
| Ulnar gutter splint | Positions the wrist and forearm in neutral with a trough along the ulnar side of the forearm. The splint is sometimes extended to position the ring and little fingers in 90 degrees of MCP flexion with IP joints in extension. | Used to support the ulnar side of the hand, wrist and forearm following fractures and dislocations. -Often used in place of a cast to accommodate edema. | A man wears an ulnar gutter splint with compression bandaging following a displaced fracture to the head of his right ulna. | 
|
| Posterior elbow splint | Positions the elbow in 90 degrees of flexion. The trough of the splint is placed along the posterior surface of the upper arm and ulnar surface of the forearm. | Used to position the elbow following fractures. | A 9-year-old girl wears a posterior elbow splint while recovering from a fracture to the olecranon process of the ulna that she sustained by falling out of a tree. |  |
| Airplane Splint | Uses a combination of rigid plastic and metal positioning bars to position the upper extremity in 90 degrees of abduction and 90 degrees of elbow flexion. Shoulder rotation and forearm/wrist/hand position is neutral. –A variation of this splint positions the elbow in full extension with the forearm in supination and the fingers extended. | Used to immobilize the shoulder following fractures or soft tissue injury. -brachial plexus injury -shoulder fractures -soft tissue injuries due to dislocation The variation that positions the elbow in extension is used to position the upper extremity following deep tissue second and third-degree burns. | A 3-year-old boy has his left shoulder immobilized using an airplane splint following a brachial plexus injury resulting from a UTV accident. | 
|
| Static finger flexion splint | Uses a static volar wrist or hand based splint with a finger sling or hook placed on or around the finger with the extension contracture. A filament is run from the finger hook or sling to a metal mount placed on the base. Tension is applied until the finger nears the end range of flexion. Tension is gradually increased as finger flexion increases. | Used to correct finger extension contractures resulting from injuries. | A woman wears a static finger flexion splint mounted to her right middle finger to correct an extension contracture resulting from an old injury sustained in a chipper/shredder accident. |  |
| Static finger extension splint | Uses a thermoplastic or metal trough with strapping to gradually stretch the finger into extension. | Used to correct finger flexion contractures resulting from injuries or neurological conditions. -Dupuytren’s contracture | A woman wears static finger extension splints on her left middle and ring fingers following surgery to release Dupuytren’s contractures. |  |
| Intrinsic plus resting splint | Places the hand in the intrinsic resting position, with the MCP joints in 90 degrees of flexion and the IP joints in full extension. | Used when the hand must be immobilized for a prolonged period. The muscles of the hand recover well from this position. | A man with a crush injury to his right hand is immobilized using an intrinsic plus resting splint and compression bandages. | 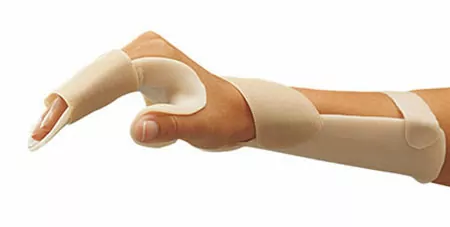 |
| Dorsal blocking splint | Places the flexor tendons of the hand in a relaxed position by preventing extension of the MCP joints. | Used to prevent stress to the flexor tendons following injury or repair. | A woman who has sustained a deep laceration to her left volar forearm wears a dorsal blocking splint while her flexor tendons heal from surgical repair. |  |
| MCP blocking splint | Holds the MCP joint in 90 degrees of flexion, facilitating PIP extension while still allowing active grasp. | Used to counteract hyperextension of the MCP joints and flexion of the PIP joints, also known as claw deformity. | A man with an ulnar nerve injury wears an MCP blocking splint to prevent ulnar claw deformity in his ring and little fingers. |  |
| Serpentine splint | Wraps in a spiral around the dorsal hand, volar thenar eminence, and forearm. | Used to counteract mild to moderate muscle spasticity in the hand, allowing for improved thumb position and increased ability to grasp. | A 9-year-old boy with cerebral palsy wears a serpentine splint on his right hand to improve his ability to grasp objects. |  |
| Thumb Abductor splint | Uses a thumb post and CMC support to place the thumb in abduction. | Helps to stabilize the CMC joint to reduce pain and improve grip and pinch strength. | A woman with rheumatoid arthritis wears a thumb abduction splint to stabilize her thumb during daily activities. |  |
.
Dynamic Splints
| Splint Name | Description | Indications | Example | Photo |
| Dynamic finger flexion splint | Provides controlled stretch to increase finger flexion but allows movement into finger extension. May use a hand or wrist base with rubber bands attached to finger hooks or finger slings. May also use a finger based spring system. Kleinert splint – combines an MCP blocking splint with rubber bands fastened to the fingernails to limit flexion while allowing dynamic extension. Used as a part of the Kleinert tendon repair protocol. |
Used to assist the recovery process after tendon and ligament injury and surgical repair. The splint is usually used to protect the repaired tendon while allowing limited movement to maintain mobility in the affected finger. | A woman wears a dynamic finger flexion splint after surgical repair to the index finger tendon of flexor digitorum profundus. |  |
| Dynamic finger extension splint | Provides controlled stretch to increase finger extension but allows movement into finger flexion. May use a hand or wrist base with rubber bands attached to finger hooks or finger slings. May also use a finger based spring system. | Used to assist the recovery process after tendon and ligament injury and surgical repair. Also used to address certain finger flexion contractures or deformities. | A 10-year-old girl wears dynamic finger extension splints on her ring and little fingers 6 weeks after a nerve graft to her ulnar nerve following an avulsion injury. |  |
| Ulnar deviation splint | Uses finger separators to position the fingers in alignment at the MCP joints. May be made out of thermoplastic or stiffened fabric. May be incorporated into the design of other hand based splints. | Used to align the fingers when the MCP joints have degenerated, causing the fingers to deviate to the ulnar side of the hand. Most common in cases of rheumatoid arthritis. | A woman with rheumatoid arthritis wears resting splints with ulnar deviation splints incorporated at night to help align and support her MCP joints. |  |
| Silver ring splints for Swan Neck deformity | Metal rings that adjust to fit over the proximal PIP joint of the finger. The rings split to provide three- point positioning, limiting hyperextension of the PIP joint. -Variations use thermoplastic or springs and finger cuffs to provide the same three-point positioning. | Used in cases of Swan Neck deformity. | A woman with rheumatoid arthritis wears silver rings splints on the index, middle and ring fingers of both hands to compensate for Swan Neck deformity. She has special ordered her splints and has incorporated gemstones on two of them to make them more attractive. |  |
| Silver ring splints for Boutonniere deformity | Metal rings that adjust to fit over the proximal and distal PIP joints, providing positioning to limit proximal PIP flexion and distal PIP extension. – Variations use thermoplastic or springs and finger cuffs to provide the same positioning. | Used in cases of Boutonniere deformity. | A man with rheumatoid arthritis wear silver ring splints on the index and middle fingers of his left hand to compensate for Boutonniere deformity. |   |
| Dynamic wrist extension splint | Uses a spring system mounted to a forearm base to maintain the wrist in extension while allowing active wrist flexion. | Used to maintain wrist position and mobility following fractures, radial nerve injury and repair, or dorsal tendon injury and repair. | A man wears a dynamic wrist extension splint while recovering from a tendon repair to extensor carpi ulnaris. |  |
| Dynamic wrist flexion splint | Uses a spring system mounted to a forearm base to maintain the wrist in flexion while allowing active wrist extension. -Some dynamic wrist splints are designed to adjust to position the wrist in either flexion or extension. | Used to maintain wrist position and mobility following fractures, median or ulnar nerve injury, or volar tendon injury and repair. | A woman wears a dynamic wrist flexion splint while recovering from median nerve graft surgery. |  |
| Soft wrist support | Made of neoprene or fabric. Provides support to the wrist and distal forearm while allowing movement in the wrist. -A variation has a thumb post for additional CMC/MCP support. | Used for conservative management of carpal tunnel syndrome and arthritis. | An elderly woman wears a neoprene wrist support to help relieve pain in her wrist resulting from osteoarthritis. |  |
| Dynamic elbow flexion/extension splint | Uses hinges and springs mounted to metal supports and plastic or fabric forearm and upper arm supports. This type of splint can usually be adjusted to facilitate or limit elbow flexion or extension while allowing limited movement within the range prescribed by the physician. | Used to aid in recovery from elbow fractures and tendon repair. Also used to reduce elbow contractures. | A man with cerebral palsy wears a dynamic elbow splint on his right arm to help reduce a severe elbow flexion contracture. |  |
| Soft elbow brace | Made of neoprene or fabric. Provides compression and support to the elbow while allowing movement. | Used to relieve pain resulting from tendonitis or arthritis.
-Lateral epicondylitis (tennis elbow) -Medial epicondylitis (golfers elbow) |
A woman wears a soft elbow brace with strapping to provide support over the tendons attaching to the lateral epicondyle to relieve pain from lateral epicondylitis resulting from her assembly line job. |  |
| Hemi-arm support | A soft shoulder support consisting of a shoulder and upper arm cuff attached to straps that fasten around the chest and shoulder girdle to hold the cuff in place. | Used to support the shoulder after tendon injury and repair, dislocation, or hemiparesis caused by CVA or TBI. | An elderly man with a diagnosis of CVA with right hemiparesis wears a hemi-arm support while walking with his therapist to prevent his right shoulder from subluxing. |  |
| Dynamic shoulder abduction splint | Positions the shoulder in varying degrees of abduction and the elbow in 90 degrees flexion. Forearm and hand positioning allows for limited forearm and hand movement. | Used to position the shoulder after injury or surgery. | A man wears a dynamic shoulder abduction splint following tendon repair to his right deltoid, which was damaged in a weight lifting accident. |  |
| Flail arm splint | Uses a shoulder harness and forearm and wrist cuffs to support the entire upper extremity and allow functional movement initiated at the shoulder. | Used to facilitate upper extremity movement following nerve injury or as a compensation technique in cases of degenerative neurological disease. -brachial plexus injury -amyotrophic lateral sclerosis -multiple sclerosis -muscular dystrophy | A boy with a 2- year history of brachial plexus injury to his left arm wears a flail arm splint to support his arm and allow for some functional movement, compensating for partial paralysis. |  |
| Tenodesis splint | A hinged splint that provides support to the thumb, index and middle fingers. The splint has a forearm base. A hinge or a wire mechanism connects the thumb/hand base to the forearm base. When the wrist is extended, the mechanism uses tenodesis action to place and hold the thumb, index and middle fingers in a closed, pinch position. When the wrist is flexed, the splint reverses the tenodesis action to open the thumb and fingers. | Used by patients with no or very limited active hand movement. Most commonly used by people with a C6 spinal cord injury. | A woman with a C6 spinal cord injury uses a tenodesis splint to help her grasp lightweight packages and dishes as she makes herself a meal. |   |
| Balanced Forearm Orthosis (Mobile Arm Support) | A device that consists of a forearm trough attached to a hinged and adjustable mounting arm. The mounting arm is attached to a wheelchair or to a fixed point at a table. The arm is adjusted to position the forearm so that when the shoulder is lowered, the elbow bends and the hand is raised toward the mouth. When the shoulder is flexed, the elbow straightens and the hand is lowered to the table. The device must be balanced properly or it will not be effective for the patient. | Used by people with upper body paralysis or extreme weakness. Must have active shoulder movement.
-C4-5 SCI |
An occupational therapist trains a woman with primary progressive multiple sclerosis how to use a balance forearm orthosis to assist hand to mouth movement so she can feed herself meals. |  |
| Suspension Sling (Deltoid Sling) | A sling that consists of an elbow support and a wrist support connected by a horizontal bar. The combination is suspended from an overhead device that is either free standing or mounted to a wheelchair. The sling supports the elbow and wrist, allowing the upper extremity to move with gravity eliminated. | Used with patients who have extreme upper extremity weakness due to acute or chronic conditions.
-CVA with hemiparesis |
A man who has sustained a left CVA with right hemiparesis uses a suspension sling to support his affected arm, allowing him to use his affected arm as an assist during light grooming and hygiene tasks while seated at a table. |  |
.
Occupational therapists use upper extremity casting to provide prolonged stretch to a joint that has developed a contracture.
There are two types of casting for contractures.
1. Serial casting: This type of casting uses casts to provide prolonged stretch to the contracted joint. A series of casts are used to gradually stretch the muscles and tissues surrounding the joint, increasing range of motion as casting progresses.
a. Used as a non-invasive treatment for contracture and/or limited range of motion in a joint.
b. Each cast is worn for 1 to 2 weeks.
c. Patients are monitored for skin integrity and tolerance of the casting process.
d. Patients may wear splints or participate in range of motion exercise programs following serial casting.
e. Common diagnoses include old soft tissue injuries, burns, cerebral palsy, CVA, TBI.
2. Inhibitory casting: Inhibitory casting uses casting to position an upper extremity affected by muscle spasticity in a function but static position. The goal of inhibitory casting is to reduce muscle tone and spasticity, resulting in reduced risk for contractures and limited range of motion.
a. The upper extremity is usually casted in a position that allows for some function.
b. One cast is applied for a prescribed period.
c. Patients may wear splints or participate in range of motion exercise programs following inhibitory casting.
Address : 11777 San Vicente Blvd, Los Angeles, CA 90049 suite # 502
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included




