SPLINTING STRATEGIES
……………… .. 
4 basic steps for designing /choosing the right splint for your patient
1. Know your upper limb conditions
2. Work out what the problem is for the patient
3. Work out how you can solve this problem
4. Decide which splint will help you achieve this goal
To help guide you through these steps, consider the following:
Purpose of splint
• Protection
• Positioning for function
• Immobilization for healing
• Restriction of undesired motion
• Correction or prevention of deformity
• Substitution of absent or weak muscles
Immobilization, restriction or mobilization
Immobilization Splints
Immobilization splints are used to protect, to prevent injury, for rest, to reduce inflammation or pain, or for positioning to facilitate proper healing after surgery.
Restriction Splints
Restriction splints limit joint ROM but do not completely stop joint motion. Semiflexible splints are available that limit motion at the extremes of range but allow motion in the middle of the range.
Mobilization Splints
Mobilization splints are designed to increase limited ROM or to restore or enhance function. A mobilizing splint may assist a weak muscle or substitute for motion lost because of nerve injury or muscle dysfunction. The splint may attempt to balance the pull of unopposed spastic muscles to prevent deformity or joint changes and to assist function. A splint may provide resistance against which a weak muscle can exercise to improve its strength or to facilitate tendon gliding after tendon surgery. Frequently, mobilizing splints are used to increase the ROM of contracted joints.
Resting vs Functional
Resting splints—generally used to immobilize the joints and provide a prolonged stretch to tight muscles.
2 types of positioning are achieved by a resting hand splint: a functional (mid-joint) position and an antideformity (intrinsic-plus/safe) position.
i. Functional position
ii. Anti-deformity (POSI) position
i. Functional Position
To rest the wrist and hand joints, the resting hand splint positions the hand in a functional or mid-joint position. This positon provides the best balance of resting length and force production so the hand can function when the patient mobilizes it again. The exact specifications of the functional position of the hand in a resting hand splint and the recommended joint positions vary.
One of the splints most frequently fabricated by OTs is the resting pan (also known as the resting hand or functional position splint), which is used to maintain the hand in a functional position. The purpose of this positioning splint is to keep the soft tissues of the hand in midrange to maintain optimal mobility and to prevent shortening of the soft tissue structures around the joints.
Wrist- 20º to 30º extension
MCP- 45º to 60º flexion
PIP and DIP- 15º to 30º flexion
Thumb- in opposition
ii. Anti-deformity/Safe position (POSI)– also known as the Intrinsic plus position, Edinburgh position and Clam digger position.
The hand can be immobilized in this position for long periods of time without developing as much stiffness as would occur if the digits were positioned differently. Commonly used for burns, trauma and invasive surgery.
Guidelines:
• MCP joints are most protected from contractures in flexion.
• PIP joints, conversely, are most protected in extension & extremely unsafe if immobilized in flexion.
POSI:
MCP flexion 70-90°
PIP in full extension
DIP in full extension
Thumb in wide abduction and opposition
Wrist extension 20-30°
Functional splints- designed to support the joints in more optimal positions for functional hand use. Functional splints are prescribed for use during activities to directly improve task performance, such as a wrist cock-up splint designed to stabilize the wrist during tasks such as handwriting.
Static vs Dynamic
A static splint has no movable components and immobilizes a joint or part of a limb. Static splints are fabricated to rest or protect, to reduce pain, or to prevent muscle shortening or contracture.
Dynamic splints are designed to protect and assist weak musculature to perform tasks, to increase passive motion, to increase active motion by assisting a joint through its range, or to substitute for lost motion. They are characterized by their mobility which is derived from resilient components (elastics, rubber bands, or springs) that produce motion. The objectives of dynamic splints are to encourage the patient to recover their mobility as quickly as possible (e.g. post surgical procedure) and thus prevent the adhesion of soft tissues, and to assist muscle imbalance in order to prevent muscular contractures and to enable the hand to rapidly regain its functional use.
| Common upper-limb conditions/deformities | Goals/Objectives | How to achieve goals | Which splint does this | Picture
|
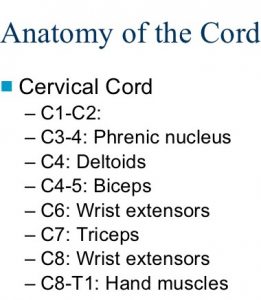
| C6 SCI
– Active wrist extension against gravity. No active finger movements.
|
Use the active wrist extension that the patient has to elicit the tenodesis effect.
When the wrist is extended, the tendons along the fingers shorten and pull the finger joints into flexion. Conversely, when the wrist is flexed the tendons along the finger joints lengthen and allow the finger joints to extend passively. |
Stabilize the thumb and hold the index and middle fingers in slight flexion. Use a static line attached to a wrist cuff to pull the finger MP joints into flexion when the wrist is extended, thus creating the ability to assume a fingertip pinch and gross grasp ability. | Tenodesis splint |  . .  |
| Brachial Plexus injury
– Upper-Trunk Injury:
|
Control pain, prevent shoulder subluxation, protect the arm from self-injury, and positon the hand in a functional position.
|
Support the entire upper extremity and enable the patient to lock their elbow in position. By providing stability at both the shoulder and elbow, the hand can be positioned for functional use. | Flail arm splint |
|
| Lateral epicondylitis (Tennis Elbow)
– Classified as an overuse injury. Most prominent symptom is pain. The extensor muscles of the forearm are involved, typically, the insertion of the extensor carpi radialis brevis. |
Provide pain relief by reducing the tension on the tendon and allowing it to heal. | A soft splint to provide compression and support to the elbow while allowing some movement. | Soft elbow brace |
|
| Hand flaccidity/palsy | Pain control, preservation of joint alignment by supporting the wrist, hand and fingers to prevent further deformity. | Position the hand in functional alignment, support the palmar arches of the hand, maintain balance between extrinsic and intrinsic muscles of hand. | Resting hand-splint in functional positon |  |
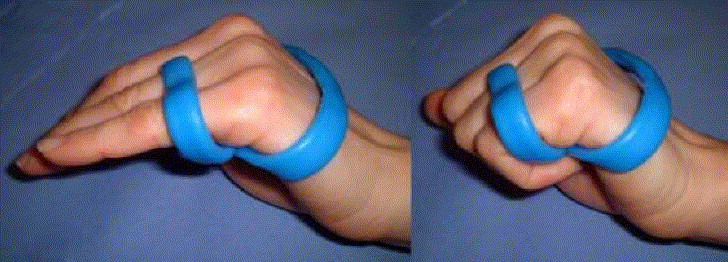
| Hand spasticity | Reduce spasticity (inhibit muscle tone by lowering the stretch reflex) and prevent contractures. | Hold the hand in a reflex-inhibiting position- Stabilize the wrist, abduct the fingers and thumb, and maintain the palmar arch.
|
Anti-spasticity ball splint |  |
| Flexion contractures of hand | Prevent further contractures from developing by maintaining the available ROM of the fingers and thumb webspace. To prevent skin maceration and breakdown, and for hygiene purposes, have a buffer between the fingers and palm. | Support the hand to retain the max opening of the hand by supporting the metacarpal arch, and protect the thenar web space from contracting. | Cone splint |  |
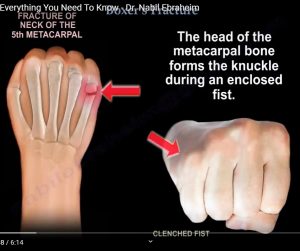
| Fracture of the 5th metacarpal
– Boxer’s fracture
|
Immobilize 4th and 5th metacarpal (ring and little fingers) to aid healing. Prevent loss of ROM of unaffected fingers and thumb, and prevent functional impairment of hand. Make accommodation for edema. |
Support the ulnar side of the hand (4th and 5th metacarpals) and wrist and, allow free movement of thumb. Position the hand in slight wrist extension, 70 to 90 degrees of flexion at MCP joints, and slight flexion at the DIP and PIP joints. Flexion of these joints is important to prevent shortening of the collateral ligaments and subsequent loss of range of motion and functional impairment.
Collateral ligaments connecting the metacarpal bones to the proximal phalanges are taut in flexion and relaxed in extension. In order to prevent shortening of the ligaments during immobilization, it is essential to immobilize the fracture in at least 70 degrees of flexion at the MCP joints. |
Ulnar gutter |  |
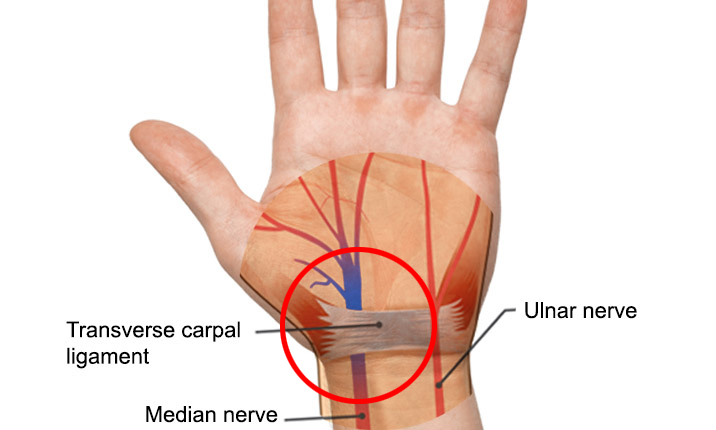
| Carpal Tunnel Syndrome
– Compression of the median nerve
|
Alleviate symptoms of pain, numbness, and tingling in the hand and prevent further damage to median nerve. | Immobilize wrist in neutral wrist position to reduce pressure on the median nerve in the carpal tunnel. | Wrist immobilization splint in NEUTRAL
* Wrist cock up splint |
  |
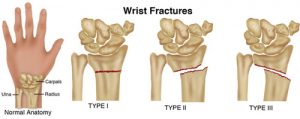
| Wrist fracture
|
Immobilize the wrist joint for restriction of motion, pain relief, joint alignment, functional support, and positioning for healing. | Stabilize and support wrist with strong support. Encompassing both volar and dorsal surfaces of the forearm allows for rigid immobilization which is excellent for fracture stabilization and strong support. | Circumferential wrist orthosis |  |
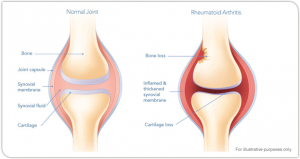
| Rheumatoid arthritis, acute synovitis
|
Provide pain and symptom relief, and prevent contractures.
– Manage pain by resting affected joints and prevent unnecessary joint motion. |
Support the wrist, fingers and thumb. Splinting should be in a position of COMFORT regardless of whether this is the ideal anatomical position. | Volar resting pan splint for hand and wrist.
** A dorsal resting pan splint is used when splint contact with the volar surface of the wrist and forearm is contraindicated. |
  |
| Ulnar drift
|
Prevent further deformity- ulnar deviation of MCP joints 2 to 5. | Align and stabilize the affected joints by maintaining a stretch on the soft tissue to increase the ROM. | Ulnar drift splint |  |
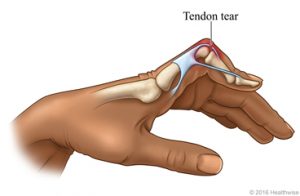
| Post-operative flexor tendon repair
|
Prevent possible tendon rupture following surgical repair. | Limit the amount of active and passive finger extension.
|
Dorsal Blocking Splint- also called a back slab splint
• Kleinert protocol • Modified Duran protocol |

|
| CMC arthritis
|
– Provide pain and symptom relief by preventing unnecessary joint motion. – Positioning for functional tasks. |
Immobilize/provide support for the CMC joint. Place thumb in a functional positon.
|
Thumb immobilisation splint |  |
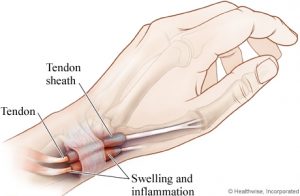
| De Quervain’s syndrome/De Quervain’s Tenosynovitis
– Painful inflammation of tendons on the side of the wrist at the base of the thumb.
|
Provide a method to rest the overused tendons and soft tissue to promote healing.
|
Immobilize thumb and wrist with a splint or brace | Long Opponens orthosis |  |
| Swan neck
– PIP hyperextension and DIP flexion
|
Prevent PIP hyperextension. | Block the PIP joint in slight flexion.
– Position the PIP joint in slight flexion to limit full PIP joint extension, but allow full PIP flexion and full DIP ROM. |
Anti-swan neck orthosis. |  .  |
| Mallet finger
– Inability to actively extend the DIP
|
Maintain the DIP joint in extension or slight hyperextension. | Hold the DIP in extension and allow functional flexion of PIP. | Mallet Finger Orthosis. | 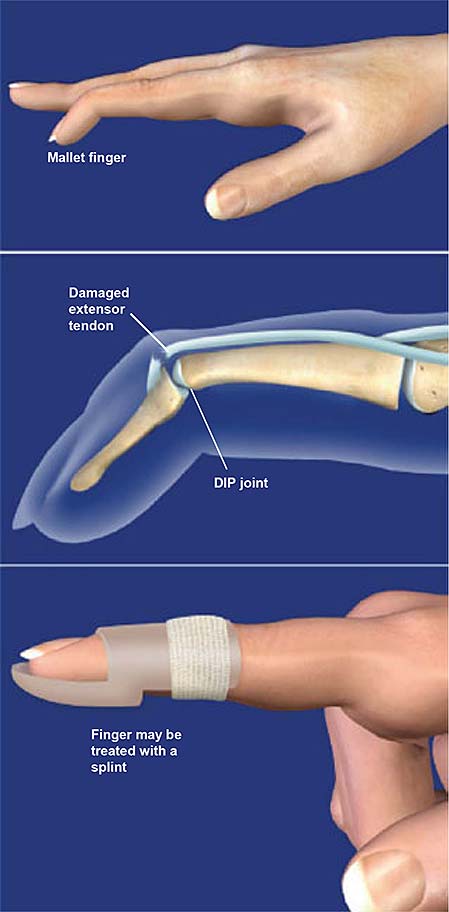 |
| Boutonniere deformity
– Extensor tendon injury characterized by PIP flexion and DIP hyperextension
|
Prevent flexion of PIP joint. Stabilize the joint to aid healing and prevent the ends of the tendon from separating as it heals. | Splint PIP joint in full extension. | PIP extension splint/silver ring. |  |
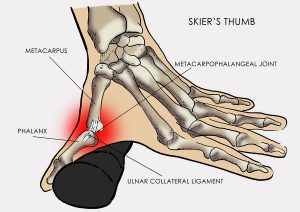
| Skier’s thumb
– Rupture of the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal joint due to a hyperabduction trauma of the thumb.
|
Pain control and prevent instability at the thumb MCP joint by avoiding putting radial stress on the thumb and giving the ligament time to heal. | Immobilize the MCP joint while allowing the IP joint to remain free to prevent unnecessary stiffness.
|
Hand-based thumb spica. |  |
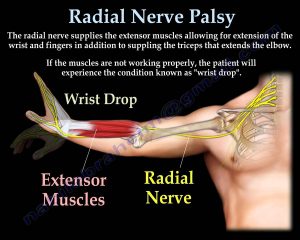
| Radial nerve palsy
– Radial nerve compression at the mid arm level is characterized by paralysis of all extensors of the wrist and digits.
|
– Substitute for loss of motor function. Compensate for loss of active wrist and finger extension to maintain joint motion and functional use of the hand. – Prevent contractures of unopposed, innervated wrist flexors. – Aid the healing process |
Allow motion while providing support- Dynamic splint.
Stabilize the wrist in a functional position (extension) and position the MCP joints, and IP joints in extension, providing controlled directional movement. Use elastics to pull the fingers back into the extended position.
|
Dynamic finger extension splint. |  |
| Median Nerve
– The Recurrent branch of the median nerve innervates muscles of the thenar eminence. Damaged with lacerations to the radial-side of wrist and proximal palm, results in loss of thumb flexion, opposition, and abduction without sensory or other motor deficits.
|
Position thumb to immobilize it for healing and to enable hand function. Keep the thumb abducted and prevent thenar web contracture. | Maintain the thumb in opposition and preserve the first web space and allow free wrist mobility. | Short Thumb Spica (Opponens) Splint, C-bar, Thumb post splint | 
|
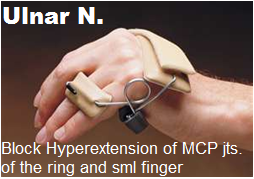
| Ulnar nerve injury
– Claw hand deformity 4th and 5th digits are hyperextended at the MCP joints and hyperflexed at the IP joints.
|
Strong extrinsic muscles lead to unopposed extension of the MCP. – Prevent hyperextension of MCPs and shortening of the MCP collateral ligaments. – Facilitate PIP joint extension, while allowing for full grasp so that maximal functional use of the hand is maintained.
|
Prevent hyperextension of MCPs by passively flexing the 4th and 5th MCP’s. Position the MCP joints in 90°of flexion. Allow active IP extension and flexion of the involved digits.
|
Static/dynamic splint to position MCPs in flexion
* Anti-claw orthosis- also known as a lumbrical blocking splint or MCP blocking splint. |
|
References:
https://www.orfit.com/physical-rehabilitation/information/#guideshttps://musculoskeletalkey.com/hand-immobilization-splints/
http://www.fixhands.com/how-to-refer/splintorthotics/
https://www.ncmedical.com/categories/Hand–Wrist_14464146.html
https://www.rehabmart.com/product/long-opponens-hand-orthosis-32934.html
https://www.slideshare.net/AbeyPRajan1/hand-rehabilitation-following-flexor-tendon-injuries
https://www.slideshare.net/StephanvanBreenenCli/occupational-therapy-and-therapeutic-technologies-interventions
http://otandsplinting.blogspot.com/2010/10/variety-of-splint.html
https://slideplayer.com/slide/246174/
https://www.slideshare.net/AndrewAntonioOTRL/091914-orthotics-project-final
Address : 11777 San Vicente Blvd, Los Angeles, CA 90049 suite # 502
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included