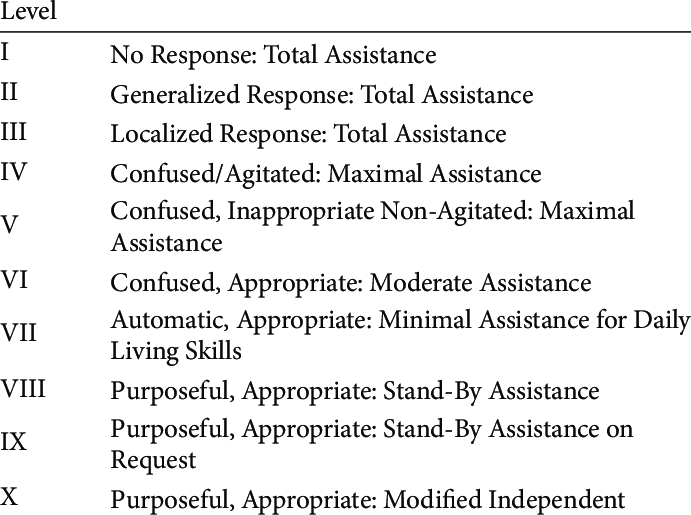
Rancho Los Amigos Levels
of Cognitive Functioning

Feb. 28, 2010: President Obama visits Cory Remsburg at the National Naval Medical Center in Bethesda, Md. (Official White House Photo by Pete Souza)
The Rancho Los Amigos Levels of Cognitive Functioning scale was developed in 1972 by Chris Hagen, PhD, Danese Malkmus, M.A. and Patricia Durham, M.A. of the Communications Disorders Services Department of Rancho Los Amigos National Rehabilitation Center in Downey, California. The scale was revised in 1974 by Danese Malkmus, M.A. and Kathryn Stenderup, O.T.R. and again in 1997 by Chris Hagen, PhD. The Rancho Los Amigos levels are designed to indicate the behavior and progression of function as the brain injury patient participates in treatment. They apply to the first few months following brain injury and are not meant to predict long term recovery. Patients may display characteristics of more than one level at a time.
Rancho I: No Response– appears to be in a deep sleep, completely unresponsive to stimuli.Stage of child development: Embryo
|
|
Rancho II: Generalized Response (vegetative state)–responses may be physiological changes, gross body movements.Stage of child development: Fetus
|
|
Rancho III: Localized Response (minimally conscious state)–responses are directly related to the type of stimulus presented.Stage of child development: Newborn
|
|
Rancho IV: Confused/Agitated–may cry out or scream–unable to cooperateStage of child development: Terrible 2’s
|
|
Rancho V: Confused, Inappropriate Non-Agitated–can usually perform self-care activities, with assistance.Stage of child development: 3 or 4-year-old
|
|
Rancho VI: Confused, Appropriate–follows simple directions consistently and shows carry-over for tasks.Stage of child development: 5 or 6-year-old
|
|
Rancho VII: Automatic, Appropriate–initiates tasks such as social or recreational activitiesStage of child development: 7-10-year-old
|
|
Rancho VIII: Purposeful, Appropriate–independent in home and community skills, including driving.Stage of child development: Teenager
|
 |
Number 2.
1,2,3 Total Assistance
4,5 Maximal Assistance
6 Moderate Assistance
7 Minimal Assistance
8 Stand By Assistance
9 Stand By Assistance on Request
10 Modified Independent
|
LEVELS 1- 3
|
TOTAL ASSIST Low motor movement Limited response to stimulation ….. Level 1– appears asleep Level 2– generalized response Level 3- localized response: turns to or away, may blink or follow object … …. |
| LEVELS
4 – 6 |
MAX ASSIST (levels 4 and 5) and MODERATE ASSIST (level 6) Confused No learning Non-goal oriented Level 4 – confused/agitated, aggressive, may crawl out of bed Level 5 – confused with agitation, inappropriate behavior, max assist with highly familiar tasks Level 6 – confused but appropriate behaviors, moderate assist with tasks, awareness up to 30 mins….. … …. |
| LEVELS
7 – 8 |
MIN ASSIST (level 7) and SB ASSIST (level 8) Automatic New learning Correct behavior with assistance Level 7 – automatic, appropriate, attends to familiar tasks up to 30 mins. unrealistic, unaware of others new learning with carry over Level 8 – Purposeful/appropriate. attends up to 1 hour. Uses lists. … ….. . |
| Level/ Description | Amount of Assistance | Behaviors and Abilities | Function: at this level, a person will display these responses. | Occupational Therapy Treatment | Video Links |
|---|---|---|---|---|---|
| I – No Response
|
Total Assistance | No observable change in behavior when presented with any kind of stimuli. | No response to any kind of stimuli, including visual, auditory or tactile input or movement. | -Passive range of motion
-Splinting and positioning to manage contractures -Sensory stimulation |
Demonstration of Level I |
| II – Generalized Response
|
Total Assistance | -Generalized reflex responses to pain
-Generalized activity responses to sound or other external stimuli -Responses may be delayed and may be the same regardless of stimuli |
Begins to respond to sensory stimuli, including visual, auditory or tactile input or movement
-Responses are inconsistent -Responses are the same to all types of stimuli -Responses are not purposeful -Responses may include chewing, sweating, changes in respiration rate, increased blood pressure, or others. |
-Passive range of motion
-Splinting and positioning to manage contractures -Sensory stimulation |
Demonstration of Level II |
| III – Localized Response
|
Total Assistance | -Reacts to pain by withdrawing or moaning
-Blinks at strong light and follows moving objects -Turns toward sound -May pull at tubes or restraints -May respond to simple commands -May respond to family or friends but not other people |
1. Awake on and off
2. Displays more movement 3. Starts reacting more specifically to different types of stimuli 4. Begins to respond to family and friends. 5. Responds to simple instructions 6. Begins to answer simple yes and no questions |
-Passive range of motion
-Sensory stimulation -Visual and auditory tracking activities -Adaptations for safety and restraint reduction |
Demonstration of Level III |
| IV – Confused/Agitated
A C C C CCCCCCCCCCCCCCCCCCCCCCCCCCCC |
Maximal Assistance | -Alert
-Heightened state of activity, may move constantly, movements not purposeful –Crying out or screaming in reaction to stimuli, out of proportion to stimuli –May run away or become aggressive –Extreme mood swings with no relation to environment -No short term memory -Unable to cooperate with treatment -Verbalizations usually incoherent or inappropriate |
1. Displays confusion and fear
2. Does not understand feelings or what is happening in surroundings 3. Responds to stimuli by acting out 4. Overly focused on basic needs, such as eating, going to the bathroom, etc. 5. Displays difficulty attending for more than a few seconds 6. Has difficulty following directions 7. Recognizes family and friends inconsistently 8. Completes simple, routine tasks with assistance |
-Active or active assistive range of motion as person will tolerate
-Simple reaching activities |
Demonstration of Level IV |
| V – Confused, Inappropriate Non-agitated
|
Maximal Assistance | -Alert, not agitated, may wander
-May become agitated in response to external stimuli -No orientation to person, place or time -Severely impaired short term memory -Uses objects inappropriately -May be able to complete familiar tasks with structure and cuing -Cannot learn new tasks -Activity often random with no direction. -No ability to problem solve or monitor own behavior -May be able to converse socially for brief periods of time with structure |
1. Pays attention for a few minutes at a time
2. Confused, difficulty making sense of anything beyond self 3. Disoriented 4. Needs step by step instructions to complete simple, everyday tasks 5. May become restless when overwhelmed or when too many people are around 6. Poor short term memory 7. May get stuck on a thought or activity and may need assistance transitioning to the next activity or step 8. Continues to focus on basic needs |
-Active or active assistive range of motion
-Simple reaching and single step fine motor tasks -Simple cognitive activities including orientation to self, place, locating own room, etc. -Basic hygiene, grooming and dressing tasks with step by step cues -Adaptations for safety, such as a bed alarm |
Demonstration of Level V |
| VI – Confused, Appropriate
|
Moderate Assistance | -Sometimes oriented to person, place and time
–Long term memory more complete than short term memory -Able to pay attention to familiar activities for up to 30 minutes with some cueing -Able to follow simple directions -Beginning to respond appropriately to family and friends -Able to complete familiar activities with supervision -Requires maximum assistance for new activities -Moderate assistance to problem solve during tasks -Vaguely recognizes staff members -Unaware of impairments, safety risk |
1. Some confusion due to memory problems. -may remember main events or main points, but will forget the details 2. Ability to follow a schedule with assistance-may become confused by changes in routine 3. Orientation to month and year 4. Attend to task for about 30 minutes. 5. Will complete basic self care tasks with help 6. May be impulsive, do or say things without thinking first 7. Will be aware of hospitalization due to injury but may not have insight into existing problems 8. Able to make sense when speaking |
-Therapeutic exercise and activity as appropriate for physical condition with direct supervision and cuing
-Cognitive activities including short term memory exercises, simple sequencing, structured single step problem solving -Basic hygiene, grooming and dressing tasks with supervision and periodic cues -Simple cold food preparation -Simple, familiar housekeeping tasks -Adaptations to immediate surroundings, including labels on drawers and closets for clothing and personal items |
Demonstration of Level VI |
| VII – Automatic, Appropriate
|
Minimal Assistance for Daily Living Skills | -Consistently oriented to person and place in familiar settings; moderate assistance to orient to time
-Minimal supervision/assistance to complete familiar tasks, including self care and household tasks -Requires minimal supervision for new learning and able to carry over new learning -Poor recall of recent activities -Superficial awareness of condition, overestimates abilities, plans for future unrealistic -Unable to determine the consequences of actions -Oppositional or uncooperative -Unaware of the needs of others; unable to recognize inappropriate social interactions |
1. Will be able to follow a schedule.
2. Will complete basic self care tasks independently 3. May have problems in new situations 4. May have problems planning, initiating, and completing activities 5. May have trouble paying attention in noisy, crowded settings or stressful situations, such as sporting events or family gatherings 6. May not be aware of how changes in memory and cognitive skills affect the future 7. Will demonstrate impaired safety awareness and judgment 8. May be inflexible, rigid in thinking, stubborn 9. May express interest in completing an activity, but may require assistance actually completing it |
-Therapeutic exercise and activity as appropriate for physical condition with initial instruction and general in-clinic supervision
–Cognitive activities including short term memory exercises, simple problem solving, decision making, basic executive function tasks -Hygiene, grooming and dressing tasks with set-up and periodic supervision -Simple cooking tasks with assistance and direct supervision, instruction in use of microwave oven, toaster -Basic housekeeping tasks -Basic home maintenance or tool use -Adaptations including labels on kitchen cupboards, closets |
Demonstration of Level VII |
| VIII – Purposeful, Appropriate
|
Stand-By Assistance | -Consistently oriented to person, place and time
-Independently attends to and completes tasks in spite of distractions -Long term and short term memory intact -May use memory devices to recall “to-do” lists or important events -Able to initiate and carry out familiar daily routines with stand-by assistance, may need minimal assistance to adapt to changes -Able to independently complete new tasks once learned -Aware of and acknowledges impairments, may need stand-by assistance to adapt or correct actions -May be depressed, irritable, argumentative, or self-centered -Over or underestimates abilities, may be overly dependent or may refuse help -Able to recognize inappropriate social interaction and correct it with minimal assistance |
1. Will realize that there is a problem with memory and cognitive skills
2. Will start to be more flexible and less rigid in thinking 3. Will begin to compensate for problems 4. Will be able to learn new information at a slower rate 5. May be ready to resume driving or undergo a return to work evaluation 6. Continues to display difficulty dealing with stressful situations 7. Will display poor judgment in new situations and may require assistance 8. May need guidance when making decisions 9. Cognitive problems may not be obvious to people who do not know the person |
-Therapeutic exercise and activity as appropriate for physical condition
-Home exercise program with repeated instruction in clinic and supervision in follow through from staff or a family member -Higher level cognitive activities including problem solving, decision making, judgment, executive function -Hygiene, grooming, dressing tasks completed independently, monitor for thoroughness -Housekeeping tasks and food preparation with set-up help, supervision, cuing to problem solve -Instruction in the use of memory aids including calendars, planners, pill organizers, timers, and other devices -Instruction and practice in energy conservation and work simplification techniques |
Demonstration of Level VIII |
| IX – Purposeful, Appropriate
|
Stand-by Assistance on Request | –Attends to task, shifts between tasks with no assistance for at least 2 consecutive hours
-Initiates and carries out all familiar routines, may request assistance -May use memory aids to recall daily schedule, “to-do” list, or important events -Able to determine the consequences of actions with assistance -Able to accurately estimate abilities but may need stand-by assistance to adjust to tasks –Able to acknowledge the needs of others and self monitor social interaction with stand-by assistance -May be depressed or irritable; low frustration tolerance |
1. Will be able to pay attention for long, sustained periods of time.
2. Aware of limitations 3. Will complete all familiar tasks 4. Will compensate for memory loss by using memory aids 5. Will consider the point of view of others during conversation 6. May return to work or daily routine with some assistance |
-Therapeutic exercise and activity as appropriate for physical condition
-Home exercise program, may complete independently after repeat in-clinic instruction -Able to complete hygiene, grooming and dressing tasks independently -Housekeeping and food preparation tasks with supervision, assist with problem solving as needed -Continued instruction in the use of memory aids -Instruction and assistance with higher level instrumental activities of daily living (IADLs), including money management, taking medications, making and keeping appointments -Assessment to determine potential to resume driving -Instruction in relaxation techniques |
Demonstration of Level IX |
| X – Purposeful, Appropriate
|
Modified Independent | –Independently carries out daily routine, may need extra time or more adaptive strategies than usual
-Able to multi-task, may need periodic breaks -Able to obtain or create own memory aids -Able to determine the consequences of actions but may need extra time or adaptive strategies to solve problems and make decision -Recognizes and appropriately responds to the feelings of others -Social interaction consistently appropriate -May become irritable or have low frustration tolerance when sick, tired or frustrated; may have periodic episodes of depression |
1. Will complete all daily activities with adaptations or extra time
2. May need rest breaks 3. Will compensate for memory loss, using adaptive aids or methods 4. Will problem solve and make decisions with extra time or adaptations 5. May become depressed or display low frustration tolerance when sick or tired 6. Will return to work or daily routine with adaptations |
-Home exercise and activity programs with follow up monitoring
-Instruct in use of and monitor follow through with memory aids, including calendars, pill boxes, alarms and timers, assistive technology -Follow up checks to insure independence with housekeeping, food preparation, safety at home -Periodic monitoring of medications, money management, appointments -Driving instruction to regain drivers license if appropriate |
Demonstration of Level X |
![]() Link between Allen Cognitive Levels & Rancho Los Amigos Scale
Link between Allen Cognitive Levels & Rancho Los Amigos Scale
| ACL | Allen Cognitive Levels | RLAS | Rancho Los Amigos |
| ACL 0 | Coma | 1 No Response
Total Assistance |
Patient does not respond to external stimuli. – No observable change in behavior when presented with any kind of stimuli. |
| 0.8 | Generalized reflexive actions | 2 Generalized Response
Total Assistance |
Patient reacts to external stimuli in nonspecific, inconsistent, and non-purposeful manner with stereotypic and limited responses. |
| ACL 1
Total Assistance |
Automatic Actions
• Automatic motor responses. Behavior is mostly reflexive |
||
| 1.0 | Withdraws from noxious stimulus | 3 Localized Response
Total Assistance |
Patient responds specifically but inconsistently to stimuli and may follow simple commands for motor actions. – Reacts to pain by withdrawing or moaning. Blinks at strong light and follows moving objects. Turns toward sound. May respond to simple commands, to family or friends but not other people. |
| 1.2 | Responds to stimuli with one sensory system | ||
| 1.4 | Locates stimuli | ||
| 1.6 | Rolls in bed | ||
| 1.8 | Raises body parts | ||
| ACL 2
Max Assistance |
Postural Actions
• Can overcome the effects of gravity |
||
| 2.0 | Overcomes gravity/sits | 4 Confused/Agitated
Max Assistance |
Patient exhibits bizarre, non-purposeful, incoherent, inappropriate behaviors. Has no short-term recall and attention is short and nonselective. Completes simple, routine tasks with assistance. Overly focused on basic needs, such as eating, going to the bathroom, etc. Has difficulty following directions. Does not understand feelings or what is happening in surroundings. – Heightened state of activity, may move constantly, movements not purposeful. May run away or become aggressive. Responds to stimuli by acting out– hitting, yelling or screaming, using abusive language, extreme behavior due to confusion, may need restraints to avoid self-injury |
| 2.2 | Righting reactions/stands | ||
| 2.4 | Aimless walking | ||
| 2.6 | Directed walking | ||
| 2.8 | Uses grab bars | ||
| ACL 3
Mod Assistance |
Manual Actions
• Uses hands to manipulate objects. |
||
| 3.0 | Grasps objects | 5 Confused, Inappropriate Non-Agitated
Max Assistance |
Alert, not agitated, may wander. No orientation to person, place or time. Absent goal directed, problem solving, self-monitoring behavior. Continues to focus on basic needs. May be able to complete familiar tasks with structure and cuing- needs step by step instructions to complete simple, everyday tasks. Uses objects inappropriately. Consistently follows simple commands. New information is not retained. -Activity often random with no direction. Cannot learn new tasks. No ability to problem solve or monitor own behavior |
| 3.2 | Distinguishes objects | ||
| 3.4 | Sustains actions on objects | ||
| 3.6 | Notes effects on objects | ||
| 3.8 | Uses all objects | ||
| ACL 4
Min Assistance |
Goal Directed Actions
Big step for independence |
||
| 4.0 | Sequences familiar actions | 6 Confused, Appropriate
Moderate Assistance |
Patient demonstrates carry-over for relearned familiar tasks (e.g. self-care) but not for new tasks. Able to follow simple directions. Able to complete familiar activities with supervision. Requires assistance for new activities. Moderate assistance to problem solve during tasks. Able to pay attention to familiar activities for up to 30 minutes with some cueing. Unaware of impairments, safety risk. – Able to complete familiar activities with supervision. Able to follow a schedule with assistance- may become confused by changes in routine. |
| 4.2 | Differentiates features of objects | ||
| 4.4 | Completes familiar goal | ||
| 4.6 | Personalizes features of objects | ||
| 4.8 | Learns by rote memorization | ||
| ACL 5
Standby Assistance/Supervision |
Exploratory Actions
• New learning can occur and can generalize skills |
||
| 5.0 | Comparing and changing variations in actions and objects | 7 Automatic, Appropriate
Minimal Assistance for Daily Living Skills |
Patient performs daily routines automatically, and shows carry-over for new learning. Will be able to follow a schedule. Will demonstrate impaired safety awareness and judgment. May express interest in completing an activity, but may require assistance actually completing it. – Minimal assistance to complete familiar tasks, including self-care and household tasks. Requires minimal supervision for new learning and able to carry over new learning. May have problems planning, initiating, and completing activities. |
| 5.2 | Discriminates parts of activity | ||
| 5.4 | Self-directed learning | 8 Purposeful, Appropriate
Stand-By Assistance |
Patient oriented and responds to the environment but abstract reasoning abilities are decreased relative to premorbid levels. Able to independently complete new tasks once learned. Independently attends to and completes tasks in spite of distractions. |
| 5.6 | Considers social standards | 9 Purposeful, Appropriate
Stand-By Assistance- on request |
Patient able to shift between tasks. Aware of limitations. Able to acknowledge the needs of others and self-monitor social interaction with stand-by assistance. Will consider the point of view of others during conversation. |
| 5.8 | Consulting with others | ||
| ACL 6
Modified- Complete independence |
Planned Actions
• No global cognitive impairment |
||
| 6.0 | Typically functioning adult brain and functional cognitive capacities | 10 Purposeful, Appropriate
Modified Independent |
Patient independently carries out daily routine, may need extra time/adaptive strategies. Will compensate for memory loss by using adaptive aids or methods. Able to obtain or create own memory aids. Able to multi-task, may need periodic breaks |
Comparing the Allen Scale of Cognitive Levels and Modes with Other Global Measures of Function- Catherine A. Earhart BA, OT Cert., OTR/L and Claudia K. Allen, MA, FAOTA, OT
https://allencognitive.com/wp-content/uploads/Ed-Corner-Comparing-Allen-Scale-with-other-Global-Measures-of-Function.pdf

At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included