
High Level Tetraplegic
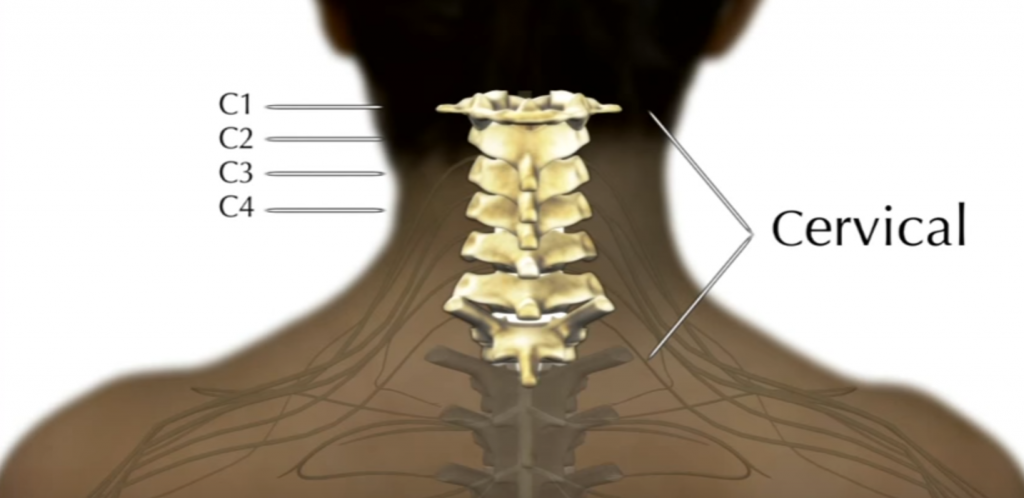
A patient with a complete C1–3 SCI is able to: speak, swallow, and control their head movement, but they do not have the ability to cough, and breathe without the support of mechanical ventilation.
Key muscle groups still working after a C1–3 spinal cord injury include:
• Sternocleidomastoid (rotates and flexes neck)
• Cervical paraspinal muscles (extend neck)
• Neck accessories (assist with speech and swallowing)
Breathing

The higher the level of injury, the greater the impact on breathing. As a complete spinal cord injury affects everything below the level of injury, this means that if the diaphragm is affected, so are the intercostal and abdominal muscles. Without the use of these muscles, a person with this level of injury cannot cough and breathe without support.
Patients with C1-C3 injuries are likely to require long-term mechanical ventilatory support because of the loss of innervation to the diaphragm. These individuals may however be candidates for functional electrical stimulation (FES) of the phrenic nerve (or diaphragm) to reduce their need for mechanical ventilation, if their lower motor innervation to the diaphragm remains intact.
If mechanical ventilation is needed long-term, surgical placement of a tracheostomy tube is performed.
There are different types of tracheostomy tubes, including:
• Cuffed versus no cuff.
• Non-fenestrated (standard tube) versus fenestrated (has a hole in the cannula that allows air to pass from the trachea through the vocal folds).
• Specialty cannula. For example, a speech cannula which has flaps for directing exhaled air to the upper airway
The Cuff
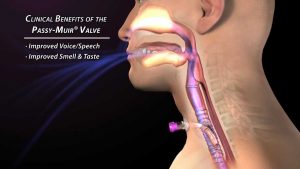
The benefits of cuff deflation include the ability to place a one-way speaking valve to allow for voice production and generation of airflow for cough and throat-clearing via the upper airway.
Swallowing
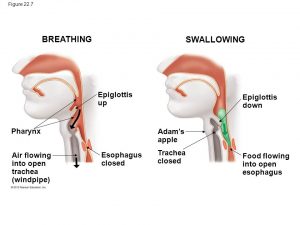
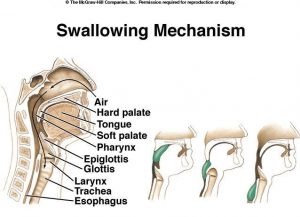
Swallowing is divided into three phases: oropharyngeal, esophageal, and gastroesophageal.
The oropharyngeal phase is controlled by the trigeminal (CN V), facial (CN VII), glossopharyngeal (CN IX), vagus (CN X), and hypoglossal nerves (CN XII).
The oropharyngeal phase is further subdivided into three stages: oral, pharyngeal, and pharyngoesophageal. The oral phase is voluntary and is controlled by cranial nerves V, VII, and XII. The food bolus is transferred into the oropharynx by the base of the tongue. Once the food bolus reaches the pharynx, the involuntary pharyngeal phase begins. Sensory receptors in the oropharynx are stimulated and via cranial nerves V, IX, and X, the swallowing reflex is initiated. To prevent aspiration the soft palate is elevated to seal off the nasopharynx and the entrance to the trachea is covered by the glottis and epiglottis. The pharyngeal phase is controlled by cranial nerves V, VII, IX, X, and XII. The final stage of oropharyngeal deglutition is the pharyngoesophageal phase. Cranial nerves IX, X, and the swallowing center in the brainstem control this stage.
Speech
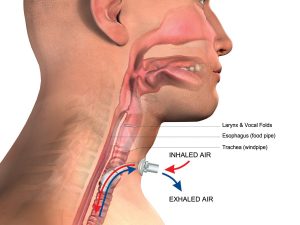
Patients on ventilators can speak as long as the tracheostomy tube allows flow through the larynx and vocal cords.
In order to talk, air moves from your lungs up through your vocal folds. The air makes the vocal folds vibrate to produce the sound that comes out of your mouth. With a trach, air goes in and out through the opening in the neck and not up through the vocal folds. The patient can however, talk if air can get through their vocal folds. Full or partial deflation of the tracheostomy cuff can allow for leakage of air across the vocal cords which will enable speech, known as “leak speech”.
Because of the design of the ventilator, speech only occurs during the expiratory cycle of the ventilator. Then there is a long silence until the next expiratory cycle and during this time, the patient will not have the air they need to speak. During this silence, the patient may lose their turn to talk. Listeners may also find it hard to follow the patient’s speech because the normal rhythm of conversational give-and-take is disrupted. Spoken phrases may have sudden bursts of loudness, reduced loudness at the end of phrases, and changes in voice quality because pressure in the trachea from the ventilator gases is not as stable as in typical speech production.
Ventilator adjustments to compensate for loss of air through the mouth and nose during cuff deflation will ensure the patient remains adequately ventilated by compensating for the leak and allowing the patient to remain stable.
It may also be possible to use a speaking valve with a ventilator. A speaking valve is a one-way valve that is placed in the trach tube and allows air to go into the patient’s trach and lungs but does not allow air to come out of the trach, instead the air comes up from the lungs, past the trach, and through their vocal cords.
Mobility- Alternative Wheelchair Control
Selecting alternative wheelchair controls is based on the individual’s abilities and personal choice.
The goal is for the patient to be able to operate a power wheelchair safely, using control devices, while maintaining optimal postural alignment.
Selecting the right control device depends on several factors, including:
1. To use a head control device the patient will need to be able to use their neck muscles efficiently to control their head movements.
2. A ‘sip and puff’ control device can only be used if the patient is able to control their breathing.
3. Neck pain and discomfort should be taken into consideration as it can be exacerbated by poor posture associated with the use of a chin control device.
4. Presence of co-morbidities -TBI associated with SCI.
Sip-n-puff
Sip-n-puff devices are widely used for controlling powered wheelchair. With a sip-n-puff system, the user gives commands to the chair by “sipping” (inhaling) and “puffing” (exhaling) on a pneumatic tube. This method works, basically, on the amount of pressure applied to the pneumatic tube and whether the sign of the pressure is negative or positive (indicating sipping or puffing, respectively). Sharp sips and puffs can be used to change the speed and direction of the wheelchair. Steering is accomplished by lower-level sips and puffs.
Head control
Head control is the option for the individuals with good head movement ability. Switches are mounted in the headrest and activated by head movement. Ideally six commands including mode and power on-off/emergency stop, as well as directional control is available.
Chin control
Chin control is considered to be different to head control. The chin sits in a cup shaped joystick handle and is usually controlled by neck flexion, extension and rotation.
Speech control
Speech systems are usually used with higher level spinal injury patients C1 – C4. The wheelchair is configured with a built-in speech recognition system which recognizes a small vocabulary of words used to control directional movement e.g. forward, back , left, right etc.
Tongue operated solution
The only commercially available tongue controller is tongue touch keypad. The system consists of 9 switches built into a dental mouthpiece. It fits in the roof of the mouth and is activated by the touch of the user’s tongue. The user can adjust the wheelchair speed by touching the front pad to go faster or the rear pad to go slower.
Using the Sip-n-Puff System


The “sip n puff” interface is a unique input method for individuals with limited mobility that interprets a user’s breath (inhaling and exhaling) using a sensor connected to a tube held in the user’s mouth. The user breathes in via the tracheostomy tube and blows out gently through the mouth.
It is possible to create enough sip and puff force to activate the system using only the facial muscles (the muscles of the cheeks, mouth and lips).

You do not use your lungs to suck through a straw, you actually create a vacuum by using the muscles in your face and pharynx. The majority of the face is composed of the buccinator muscle, which compresses the cheek. Lateral movement of the cheeks enables you to suck on a straw, compress air in your mouth to blow out, whistle, and contributes to the action of chewing (accessory muscle of mastication).
Jenni Taylor, C1-C2 Quad, explains the logistics of traveling as a vent-dependent quad
Resources:
http://atwiki.assistivetech.net/index.php/Alternative_wheelchair_control
https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-64402008000200008
https://www.sciencedirect.com/topics/agricultural-and-biological-sciences/deglutition
https://www.asha.org/public/speech/disorders/tracheostomies-or-ventilators/
https://www.hopkinsmedicine.org/tracheostomy/living/passey-muir_valve.html
https://breathe.ersjournals.com/content/12/4/328
Address : 11777 San Vicente Blvd, Los Angeles, CA 90049 suite # 502
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included

