
Functional Independence Measure (FIM)
Quick Reference Guide
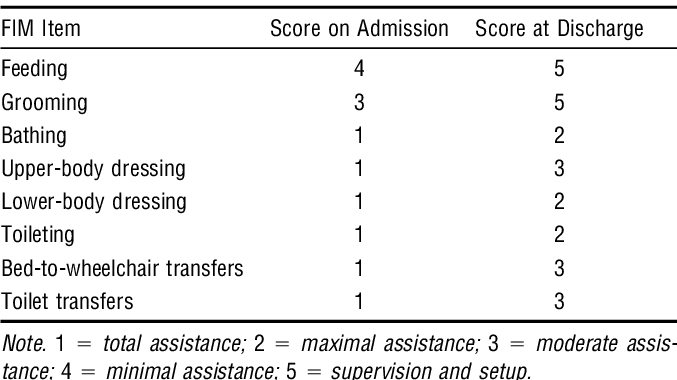
The Functional Independence Measure, or FIM, is an assessment tool used to track outcomes in hospitals and skilled nursing facilities. The following charts will review the functional levels of the FIM and what the numbers mean in terms of a patient’s level of independence.
Motor Tasks
Activities of Daily Living
| Activity | 7 – Complete Independence | 6 – Modified Independence | 5 – Supervision or Set Up | 4 – Minimal Contact Assistance (performs >75% of task) | 3 – Moderate Assistance (performs 50 – 74% of task) | 2 – Maximal Assistance (performs 25 – 49% of task) | 1 – Total Assistance (performs < 25% of task) | 0 – Activity Does Not Occur |
| Eating | Does not need help or any modifications | Needs assistive device, increased time, or modified consistency of food. | Needs cuing or set-up. Help required to open containers, pour liquids, cut food. Monitoring for safety issues. | Needs incidental assistance such as placement of food or scoop food. | Needs physical assist to eat, such as physical guidance hand to mouth. | Needs maximum physical assist – may be able to drink from a straw or wipe mouth. | Dependent during feeding or tube fed. | Entered only for admission assessment if patient does not receive any nutrition during assessment (rare). |
| Grooming | Does not need help or any modifications. | Needs assistive device, increased time, or adaptations for safety issues. | Needs cuing, encouragement, or assistance organizing grooming supplies. Needs direct supervision for safety. | Needs incidental assistance or help with specific tasks (i.e. help applying toothpaste). | Needs physical assistance for all grooming tasks but able to participate. | Needs significant physical assistance to participate. | Dependent but may be able to position face or hold washcloth. | Entered only for admission assessment if patient does not perform any grooming activities (rare). |
| Bathing | Does not need help or any modifications. | Needs assistive device, increased time, or adaptations for safety issues. | Needs cuing, encouragement, or assistance setting out bathing supplies. Needs direct supervision for safety. | Needs incidental assistance such as placement of washcloth. | Needs physical assistance to bathe one or two areas (i.e. help washing back). | Needs physical assistance to bathe most areas but able to participate by positioning limbs, standing or turning. | Dependent helper performs most or all of the task. | Entered only for admission assessment if patient does not bathe self or is not bathed by helper. |
| Dressing | Does not need help or any modifications. | Needs assistive device, increased time, or adaptations for safety issues. | Needs assistance selecting and setting out clothing. Needs direct supervision for safety. | Needs incidental assistance adjusting clothing, fastening difficult fasteners. | Needs physical assistance to put on or remove one or two clothing items, assistance to fasten all fasteners. | Needs physical assistance to put on or remove all clothing items, able to participate by positioning limbs, standing or turning. | Dependent helper performs most or all of the task. | Entered only for admission assessment if patient does not dress self or is not dressed by helper. |
| Bowel and Bladder Management | Does not need help or any modifications. | Needs assistive device, equipment, pads, or medication. | Needs cuing, encourage-ment or assistance to set up equipment. | Needs incidental assistance such as placing equipment, adjusting clothing. | Needs physical assistance for more than one task or to manage equipment. | Needs physical assistance for all tasks but able to participate by positioning body. | Dependent helper performs most or all of task and manages equipment. | Entered only for admission assessment if patient does not manage bowel or bladder or is not assisted by helper. |
| Bowel and Bladder Management, Part II: Frequency of bowel or bladder accidents over the past 7 days. | No accidents. | No accidents, using assistive device, equipment, pads or medication. | 1 accident, including bedpan or urinal spills. | 2 accidents, including bedpan or urinal spills. | 3 accidents, including bedpan or urinal spills. | 4 accidents, including bedpan or urinal spills. | 5 or more accidents, including bedpan or urinal spills. | Entered only for admission assessment if patient does not have a bowel movement or does not urinate. |
| Toileting – includes perineal hygiene and clothing management before and after use of toilet or bedpan | Does not need help or any modifications. | Needs assistive device or more time to complete | Needs cuing, encourage-ment or assistance to set up equipment. Needs direct supervision for safety. | Needs incidental assistance such as physical support for balance while performing hygiene or adjusting clothing. | Needs physical assistance for more than one task or to manage equipment. | Needs maximum physical assistance but can participate by positioning body. | Dependent helper performs most or all of task and manages equipment. | Entered only for admission assessment if patient does not use the toilet or bedpan. |
Mobility
| Activity | 7 – Complete Independence | 6 – Modified Independence | 5 – Supervision or Set Up | 4 – Minimal Contact Assistance (performs >75% of task) | 3 – Moderate Assistance (performs 50 – 74% of task) | 2 – Maximal Assistance (performs 25 – 49% of task) | 1 – Total Assistance (performs < 25% of task) | 0 – Activity Does Not Occur |
| Transfers: Bed, Chair, Wheelchair in both directions. Toilet and Tub are scored separately. | Does not need help or any modifications. | Needs assistive device such as grab bar, sliding board, or needs extra time. | Needs cuing, encourage-ment or assistance to set up equipment. Needs direct supervision for safety. | Needs incidental assistance such as placement of equipment, physical contact for safety. | Needs physical assistance for balance, changing direction, or adjusting position. | Needs maximum physical assistance but may be able to participate by positioning limbs, partially supporting weight. | Dependent helper performs most or all of task and manages equipment. | Entered only for admission assessment if patient does not transfer or is unable to get out of bed (rare). |
| Locomotion: Walk or Wheel-chair, to be scored on level surfaces. | Walks >150 feet. Does not need help or any modifications. | Walks >150 feet. Needs assistive device. | Walks >150 feet. Needs cuing , encouragement, or assistance to set up equipment. Needs direct supervision for safety. | Walks > 150 feet. Needs incidental assistance such as contact guard or steadying. | Walks >150 feet. Needs physical assistance such as hand hold or physical assistance to swing foot. | Walks 50 – 149 feet. Needs one person physical assistance to perform task. | Walks < 50 feet. Needs 2 person physical assistance to perform task. | Entered only for admission assessment if patient does not walk or use wheelchair. |
| Stairs: Scores to ascend or descend one flight of stairs. | 12-14 stairs. Does not need help or any modifications. | 12-14 stairs. Needs assistive device. | 12-14 stairs. Needs cuing, encouragement, or assistance to set up equipment. Needs direct supervision for safety. | 12-14 stairs. Needs incidental assistance such as contact guard or steadying. | 12-14 stairs. Needs physical assistance for a portion of the task, such as initiating step down. | 4-6 stairs. Needs 1 person maximum physical assist to perform task. | Less than 4 stairs. Needs 2 person maximum physical assist to perform task. | Entered only for admission assessment if patient does not climb up or down stairs |
Cognitive Tasks
| Activity | 7 – Complete Independence | 6 – Modified Independence | 5 – Supervision or Set Up | 4 – Minimal Contact Assistance (performs >75% of task) | 3 – Moderate Assistance (performs 50 – 74% of task) | 2 – Maximal Assistance (performs 25 – 49% of task) | 1 – Total Assistance (performs < 25% of task) |
| Comprehension: Understands auditory and/or visual communication, including basic (pain, hunger, etc.) and complex (current events, finances, etc.) | Understands complex or abstract information. | Understands most situations readily or with mild difficulty. Does not need prompting and can self-correct. | Understands directions and conversations about basic needs 90% of the time or more. | Understands directions and conversations about basic needs 75 – 89% of the time. | Understands directions and conversations about basic needs 50 – 74% of the time. | Understands directions and conversations about basic needs 25 – 49% of the time. | Understands directions and conversations about basic needs less than 25% of the time. May understand simple common expressions. |
| Expression: Includes clear vocal and/or non-vocal expression of language | Expresses complex or abstract ideas. | Expresses complex ideas in most situations readily or with mild difficulty. Does not need prompting and can self-correct. | Expresses basic daily needs and ideas 90% of more of the time. | Expresses basic daily needs and ideas 75 – 89% of the time. | Expresses basic daily needs and ideas 50 – 74% of the time. | Expresses basic daily needs and ideas 25 – 49% of the time. Uses only single words or gestures. | Expresses basic daily needs and ideas less than 25% of the time. |
| Social Interaction: Cooperates, gets along with staff, family and other patients | Appropriate social interactions. | Appropriate interactions most of the time. May require extra time and/or medication. | Needs supervision during stressful situations. Interacts appropriately 90% of more of the time. | Interacts appropriately 75 – 89% of the time. | Interacts appropriately 50 – 74% of the time. | Interacts appropriately 25 – 49% of the time. | Interacts appropriately less than 25% of the time. |
| Problem Solving: Participates in decisions regarding personal, financial, and social activities. | Able to recognize, initiate and carry out steps to solve complex problems. | Recognizes and resolves most problems. May need more time. | Requires assistance to solve less routine problems 10% of the time. | Solves routine problems 75 – 89% of the time. | Solves routine problems 50 – 74% of the time. | Solves routine problems 25 – 49% of the time. | Solves routine problems less than 25% of the time. May require 1:1 assistance. |
| Memory: Recognizes familiar faces, recalling routine and complex situations. | Able to recall routine and remember complex requests. | May use cues or aids to help recall. | Needs cueing only in new or stressful situations. | Recalls people and routine 75 – 89% of the time. | Recalls people and routine 50 – 74% of the time. | Recalls people and routine 25 – 49% of the time. | Recalls people and routine less than 25% of the time. May require 1:1 assistance. |
.
Occupational Therapy Treatment Based on FIM Levels
| Level | Treatment | Examples | Video |
| 1 – Total Assistance, performs <25% of task. | -Passive range of motion or active-assistive range of motion if conscious. -Hand over hand assistance for simple grooming tasks. -Splinting and positioning to prevent contractures and pressure ulcers. -Sensory stimulation activities. |
An occupational therapist provides passive range of motion and fabricates resting pan splints for an end stage multiple sclerosis patient. An occupational therapist adapts a wheelchair to include a pressure relieving cushion and pelvic positioning for a woman with advanced Alzheimer’s disease. |
A description of the FIM scale as used by Waverly Glen. |
| 2 – Maximal Assistance – performs 25 – 49% of task | -Active-assistive range of motion and simple active-assistive reaching activities. -Self feeding and simple grooming tasks with physical assistance to initiate movements. -Dressing tasks with prompts to position limbs. -Simple memory stimulation activities – watch old movies, look at pictures with prompts and physical assistance to turn pages. |
An occupational therapist provides hand over hand assistance to a woman with generalized weakness to brush her hair. An occupational therapist helps a man with a severe developmental disability to wash his face by placing the washcloth in his hand and providing hand over hand assistance to move the cloth while he holds it. |
Occupational therapy students demonstrate the FIM levels for lower body dressing. |
| 3 – Moderate Assistance – performs 50 – 74% of task | -Active assistive range of motion or active range of motion with assistance for end ranges. -Simple reaching activities. -Simple one-step fine motor tasks. -Basic ADL tasks with set-up and physical assistance to initiate movement, physical assistance with tasks requiring more complex movements such as fastening clothing fasteners. -Simple memory tasks and games with prompting. |
An occupational therapist has a man with severe rheumatoid arthritis slide his arms on a table top, using a towel to reduce friction, to perform shoulder stretching exercises. An occupational therapist helps a man with senile dementia feed himself breakfast by providing him physical assistance to scoop his oatmeal with a spoon, then allowing him to lift the spoon to his mouth without physical assistance. |
Occupational therapy students demonstrate the FIM levels for bathing. |
| 4 – Minimal Assistance – performs >75% of task | -Active range of motion and simple strengthening exercises with assistance to keep track of repetitions. -Basic fine motor tasks. -Basic ADL tasks with physical assistance for more complex steps such as donning and tying shoes, fastening clothing fasteners, adjusting clothing. -Simple housekeeping tasks, such as wiping counters, sweeping. -Guided leisure activities – bingo, Wii games, familiar individual hobbies with assistance. |
An occupational therapist helps a man recovering from a hip fracture to place his feet in his pants, then steadies him to stand while he pulls the pants up. An occupational therapist helps a woman with mild dementia to thread a needle and start a piece of cross-stitch, a hobby the woman has participated in for many years. |
Occupational therapy students demonstrate administration of the FIM, using the FIM decision tree to score upper body dressing, lower body dressing, and grooming. |
| 5 – Supervision or Set-up | -Active range of motion, strengthening exercises with set-up, visual demonstration, verbal prompts. -Therapeutic activities with set-up and supervision. -ADL tasks with assistance to gather grooming and hygiene items, select and obtain clothing, prompts for thoroughness. -Light housekeeping tasks with supervision, prompts for thoroughness. -Simple food preparation with assistance to gather needed items, supervision for safety. |
An occupational therapist supervises a man recovering from a stroke as he completes pulley exercises, giving him periodic prompts to count repetitions. An occupational therapist supervises a woman recovering from pneumonia as she prepares cold food in the OT kitchen, prompting her to use energy conservation techniques as she works. |
Occupational therapy students demonstrate administration of the FIM for transfers, mobility, and toileting. |
| 6 – Modified Independence | -Education in the use of adaptive equipment and adaptive techniques. -Set-up and training in home range of motion and strengthening programs. -Education in energy conservation, joint protection, work simplification techniques. -IDAL assessment and home evaluation prior to return to home. |
An occupational therapist collaborates with a physical therapist to evaluate and provide recommendations for adaptations to the home of a man who is returning home after hip replacement surgery. An occupational therapist trains a woman with severe rheumatoid arthritis in joint protection techniques during a cleaning task. |
An occupational therapy student demonstrates how to administer the FIM for grooming, upper body dressing and eating. |
| 7 – Complete Independence | Occupational therapy is usually discontinued at or before this level. | Occupational therapy is no longer required – patients are independent in all tasks at this level. | A student study group applies the FIM to case scenarios. |
.
Many inpatient facilities use the FIM to track patient outcomes. From this tracking, facilities can obtain data to determine how effective their nursing and rehabilitation programs are in helping patients to return to independence. Here is an example of what FIM tracking for a man recovering from a hip fracture might look like. (The man is independent in all cognitive areas.):
| Date | Eating | Grooming | Bathing | Dressing | Bowel/Bladder 1 | Bowel/Bladder 2 | Toileting | Transfers | Locomotion | Stairs |
| Admission | 5 | 5 | 2 | 2 | 1 (catheter) | 3 | 1 | 1 | 1 | 1 |
| Week 1 | 5 | 5 | 3 | 3 | 3 (catheter removed) | 5 | 3 | 3 | 2 | 1 |
| Week 2 | 7 | 6 | 4 | 4 | 4 | 6 | 4 | 4 | 3 | 2 |
| Week 3 | 7 | 7 | 5 | 5 | 5 | 7 | 5 | 5 | 5 | 3 |
| Week 4 | 7 | 7 | 6 | 6 | 6 | 7 | 6 | 5 | 5 | 4 |
| Discharge | 7 | 7 | 6 | 6 | 6 | 7 | 6 | 6 | 6 | 5 |
When the man is discharged from the facility, he must use a walker for mobility but can do so independently. He must also use a reacher, sock aide and long shoe horn to complete lower body dressing, but can also do this independently. He continues to display some difficulty managing stairs, so the physical therapist recommends that he be supervised when he is on stairs. Notice that upon discharge, those tasks that the man requires adaptive equipment to complete are rated a 6 rather than a 7. Stairs are rated a 5.
Address : 11777 San Vicente Blvd, Los Angeles, CA 90049 suite # 502
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included

