
A Traumatic Brain Injury (TBI) is a complex injury with varying symptoms and disabilities. It ranges from a brief alteration of consciousness in mild cases to prolonged unconsciousness or death in severe cases. This condition often results from the brain being harmed by a mechanical force, such as a rapid acceleration-deceleration or a direct impact.
TBI Severity Classification
Understanding TBI severity is crucial for effective treatment. The Glasgow Coma Scale (GCS) is a primary method for classifying TBI severity:
- Severe TBI: GCS score of 3-8
- Moderate TBI: GCS score of 9-12
- Mild TBI: GCS score of 13-15
In our full guide, we delve further into GCS with case examples and explain how it impacts treatment strategies.
Classification of TBI
TBIs are categorized further into primary and secondary injuries:
- Primary Injury: Occurs at the time of the trauma.
- Secondary Injury: Occurs as a result of physiological response to the initial injury.
Within these categories, TBIs can also be focal, like skull fractures, or diffuse, like diffuse axonal injury.
TBI Levels and Symptoms
The different levels of consciousness and cognitive functions after a TBI can be understood through scales like Rancho Los Amigos Scale. Symptoms vary greatly and can include:
- Vomiting
- Lethargy
- Confusion
- Paralysis
- Vision changes
- Speech difficulties
Vegetative State Symptoms
Understanding symptoms associated with states of consciousness like the vegetative state, where patients appear awake but are unaware of themselves or their environment, is essential.
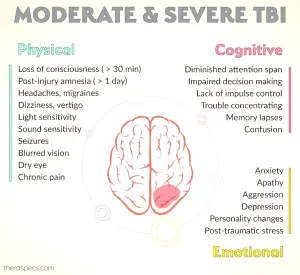
Moderate TBI Symptoms
Moderate TBIs often present symptoms such as confusion, headache, and balance issues. Effective management of these symptoms involves comprehensive rehabilitation plans.
OT Interventions for TBI
Occupational Therapy (OT) interventions play a critical role in TBI recovery:
- Motor function improvement: Rehabilitation programs focus on balance and coordination.
- Improving ADLs: Activity-based interventions tailored to individual goals.
- Enhancing self-awareness: Video feedback helps in acknowledging deficits.
- Memory strategies: Techniques like self-generation aid in better retention.
Explore more OT strategies in our comprehensive guide, which includes practical exercises and case studies.
Want detailed practice tips to ace the NBCOT® exam? Join now for full access!

