
What Causes Down Syndrome?
Down syndrome is a chromosomal condition associated with intellectual disability. It results from an accident in cell development leading to 47 chromosomes instead of the usual 46. This extra chromosome alters the development of the body and brain. The condition is generally diagnosed shortly after birth through chromosome tests.
Incidence and Demographics
- Occurs in 1 in 1,000 live births.
- Higher likelihood in children born to mothers over 35 years of age.
- Accounts for 20% of Down syndrome births although only 5 to 8% of pregnancies occur in women over 35.
Down syndrome occurs across all cultures and demographics, indicating there is no single cause of Down syndrome influenced by environment or ethnicity.
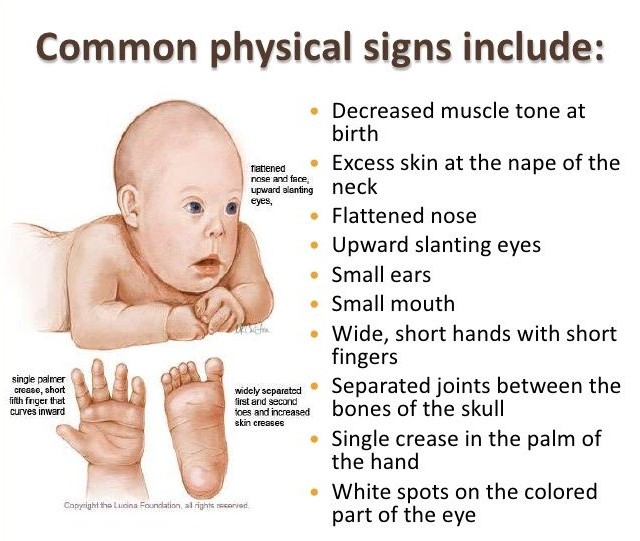
Down Syndrome Symptoms and Features
Physical Characteristics
- Flat-bridged nose and slanting, almond-shaped eyes.
- Protruded abdomen and short stature.
- Short fingers and limbs, and a tendency to be overweight.
- Slanted eyes and a small oral cavity with a protruding tongue.
- Structural abnormalities in the lungs and airway.
Understanding the features of Down syndrome helps in providing timely interventions for related health issues.
Motor and Sensory Challenges
Children with Down syndrome may exhibit decreased kinesthetic awareness and balance, leading to challenges in activities requiring physical coordination.
Associated Health Risks
- 40 to 60% may have congenital heart disease.
- Increased susceptibility to pulmonary problems.
- Vision and auditory challenges affecting learning and development.
Teaching Tips for Students with Down Syndrome
- Adapt cardiovascular and agility activities to individual needs.
- Utilize alternative communication methods as necessary.
- Incorporate family into devising and executing solutions.
- Encourage muscle strengthening, especially around joints.
- Emphasize personal care, nutrition, and appropriate activity levels.
Recognizing and Managing Atlantoaxial Instability (AAI)
AAI is increased mobility between the first and second cervical vertebrae. It affects 15% of children with Down syndrome but often remains asymptomatic without subluxation. Monitoring through x-rays and symptom awareness is crucial.
Signs of AAI include:
- Changes in bowel or bladder function.
- Difficulty in walking or neck pain.
- Progressive clumsiness and coordination loss.
- Require adherence to physician’s activity guidelines and medical records access to ensure safe participation in physical activities.
For an in-depth exploration, our full guide dissects key characteristics of developmental groups with real-life examples and quizzes.
Want detailed practice tips to ace the NBCOT® exam? Join now for full access!

