
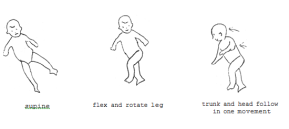
Primitive Reflexes and Postural Reactions …….. ………. …. ……….. Primitive Reflexes Postural Reactions 1. Righting reactions (RR) 2. Equilibrium reactions (ER) 3. Protective reactions Place in quadruped; cervical flexion with chin tuck. Arms flex, legs extend ** Segmental rolling develops at about six months of age and is a mature adaptation of the neck righting reflex and the body righting reflex. As its name suggests, rather than the body moving as a whole, rotation takes place at the central axis of the body and the shoulders and pelvis move separately. If the rolling movement starts with head rotation, the shoulders will follow, and then the pelvis. The movement can also be initiated from the opposite direction, at the pelvis. Postural Reactions
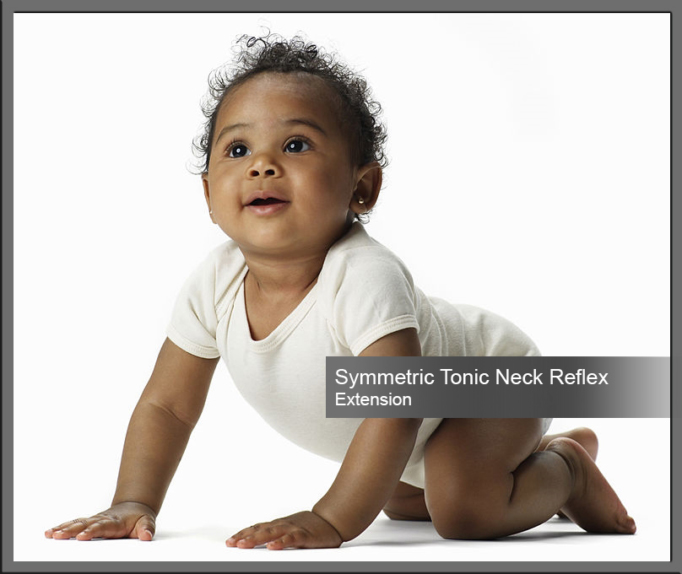
Testing Reflexes and Postural Reactions ATNR This newborn reflex is elicited by holding the newborn in ventral suspension (face down) and run a finger down one side of the spine. The normal reaction is for the newborn to laterally flex toward the side that was stroked. STNR Forms the bridge from lying to crawling on hands and knees. In addition STNR helps the child develop near/far fixation. With head and arms extended (STNR Extended) the child can fixate on far away objects. Head down with legs extended ( STNR Flexion) the child has a near fixation. The child’s first response to the forces of gravity. This reflex is seen when moving the child’s head in towards their body (position in utero) causes the arms and legs to also move in. Extension of the head above/below the spine causes extension of the arms and legs. By 6 months of age this is modified so the child will develop head control through oculomotor and head-righting reflexes.
Retained Primitive Reflexes Primitive Reflexes which are not integrated within the expected/typical developmental time period are known as: Persistent or Retained or Uninhibited Reflexes Primitive reflexes are involuntary muscle movements that originate from the brainstem and executed without cortical involvement. They develop in-utero and are essential during the first few months of life for the infant’s survival. In typical development, during the first year, these reflexes naturally become inhibited in a sequential order. As the primitive reflexes are inhibited, they are replaced with postural reflexes which are more mature patterns of response that ultimately control balance, coordination and sensory motor development. New skills are acquired, and higher centers of the brain begin to mature and develop. Reflex Integration refers to the inhibition of the reflexes by the higher centers of the brain which modify the reflex in such a way that the pattern of response is no longer stereotypical. If primitive reflexes are retained beyond 12 months of life, they suggest evidence of a structural weakness or immaturity of the CNS. Their presence is therefore considered as being an indication that underlying neurological issues may exist. When these reflexes do not integrate, they may interfere with a child’s development of more advanced motor skills. Children who have Neurodevelopmental disorders e.g. ADD/ADHD, Sensory Processing Disorders, ASD, or learning disorders typically have retained primitive reflexes that can contribute to their symptoms and affect their learning and behavior.
Automatic stereotypic movements in response to specific stimuli. They are controlled by the brainstem and therefore require no cortical involvement. These reflexes are necessary for the survival and development in the womb and in the early months of life. However, as higher more sophisticated centers of the brain begin to mature, these primitive reflexes become integrated in order for proper neurological organization of the brain to develop.
Maturational motor skills that develop during the first year of life and form the basis for attainment of functional motor skills. Postural reactions respond to more global stimuli than primitive reflexes and last for a lifetime, in order to support movement and balance. The effects of gravity on the body, triggers postural reactions.
There are 3 Types of Postural Reactions
1. Righting reactions
2. Equilibrium reactions
3. Protective reactions
Righting reactions support positioning of the head vertically in space, alignment of the head and trunk, and alignment of the trunk and limbs.
Righting reactions can be broken into five different reflexes that serve to keep the head in a normal position, right the body to a normal position and adjust the body parts in relation to the head and vice versa.
i. Labyrinthine righting reflexes acting on the head/Head righting reflex
ii. Body-righting reflexes acting on the head (BOH)
iii. Neck-righting reflexes (NOB)
iv. Body-righting reflexes acting on the body (BOB)
v. Optical righting reflexes
ER provide balance when the center of gravity is disturbed. They are more mature responses to regain balance than righting reactions. They consist of complex responses which seek to restore disturbed balance. Movement of the trunk and extremities in a direction opposite to the force which is causing displacement, is elicited.
This reaction involves movements of extension of the extremities in the same direction as the displacing force. Protective reactions are required to prevent injury if the equilibrium reactions are unable to restore balance. Protective reactions emerge first to the front, then the side and then backwards . Primitive Reflexes
Reflex
Purpose
Position/Stimulus
Positive reaction
Onset/Integration Age
Rooting

Searching for food
Stroke corner of mouth.
Movement toward stimulus
28 wks g → 3mos
Suck-swallow
Ingestion of food
Place finger inside mouth.
Rhythmic sucking
28 wks g → 2-5mos
Traction

Stabilize head prior to voluntary control
Grasp infants forearms & pull-to-sit
Complete flexion and elevation of upper extremities
28 wks g → 2-5mos
Moro “infant startle reflex”
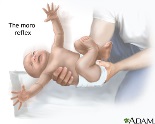
Involuntary response to sudden change in stimuli. If it persists can cause hypersensitivity, easily trigger emotional outbursts; etc.
Rapidly drop infants head backwards
• Phase 1: arm extension/abd & hand opening
• Phase 2: arm flex & add28 wks g → 4-6mos
Plantar grasp
↑ tactile input to foot.
Pressure using thumb on ball of foot
Toe flexion
28 wks g → 9mos
Galant

Helps with balance and coordination for crawling and creeping; connected to bladder function → ↑ % of bedwetters past 5yrs of age have active galant reflex.
Hold infant in prone suspension; scratch or tap alongside the spine w/ finger, from shoulder to butt
Lateral trunk flexion & wrinkling of the skin on the stimulated side
32 wks g → 2mos
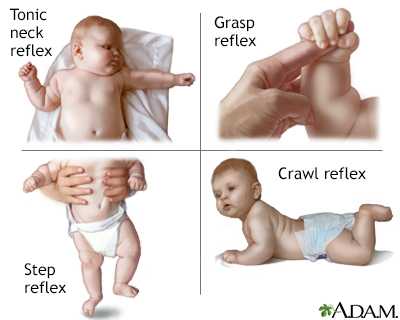
Asymmetric tonic neck

Eye hand coordination; one-handed movements.
Supine; Turn head to side.
Extension of extremities on the face side, flexion of extremities on the skull side
37 wks g → 4-6mos
Palmar Grasp
Development of grasp; if it persists can hinder development of grasp and release patterns.
Place finger in palm
Finger flex; reflexive grasp
37 wks g → 4-6 mos
Tonic labyrinthine-supine (TLR)
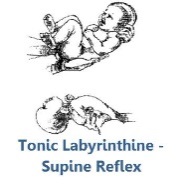
Extensor tone;
Increase extensor tone, practice balance; prop awareness, posture, coordination, head alignment.Supine; passively flex legs and arms
↑ extensor tone
> 37 wks g → 6mos
Tonic labyrinthine-prone (TLR)
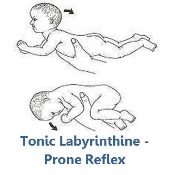
Flexor tone; Increase flexor tone, practice balance; prop awareness, posture, coordination, head alignment.
Prone;
↑ flexor tone
> 37 wks g → 6mos
Labyrinthine/optical (head) righting

Orients head in space; allows body to turn while maintaining upright position of head.
Hold infant vertically and tilt to the side, forward, or backward
Vertical position of head; head steady.
Birth-2 → Persists
Landau “Superman”

Breaks up flexor dominance.
prone suspension
Complete extension of head, trunk, and extremities “superman”
3-4 mos → 12-24mos
Symmetric tonic neck (STNR)
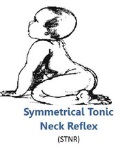
Precursor for crawling/creeping
Place in quadruped; cervical extension .
Arms extend, legs flex.
4-6 mos → 8-12mos
Neck righting (NOB)

Initiates Rolling. (transition btw supine, side-lying, & prone)
Place infant in supine, turn head to one side
Entire body turns in direction of head.
4-6 mos → 5yrs
Body righting (BOH)
Helps rolling btw supine, side-lying & prone
Place in supine, flex hip/knee over chest.
Upper body follows pelvis in log roll.
4-6 mos → 5yrs
Babinski
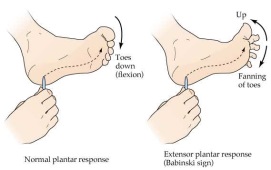
Children>2 = disorder. Seen in MS, ALS, Stroke.
Foot stroked (heel to base of toes)
Ext. of big toe, other toes will fan out.
Birth → 1yr
Reflex
Purpose
Stimulus
Response
Onset/Integration Age
Downward parachute (protective extension downward)

Prep for standing; breaking fall.
Suspended vertically, child usually held under arms in vertical suspension and lowered rapidly to simulate a falling sensation
Extension of lower extremities
4 mos → Persists
Forward parachute (protective extension) forward

Prep for sitting; breaking/preventing fall.
Suddenly tip infant forward while vertically suspended. Infant held under the arms at mid-thorax and tilted forward.
Extension of the UEs, hand opening, and neck extension “about to break a fall”
6-9mos → Persists
Sideward parachute (protective extension sideward)
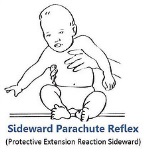
Prevent fall; increase support (arm extension) on side opposite force- stop from falling to side.
Tip infant off-balance to side.
Arm extension and abd to the side
7 mos → Persists
Backward parachute (protective extension sideward)
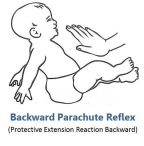
Prevent fall
Tip infant off-balance backward
Backward arm extension
9-10mos → Persists
Prone tilting
Maintain balance w/out arms; postural adjustments
Use tilt board. Infant in prone; raise one side.
Spine curves toward raised side); ext/abd of all 4 extremities.
5 mos → Persists
Spine tilting & Sitting tilting
Maintain balance w/out arms; postural adjustments
Use tilt board. Infant in sitting or supine; raise one side.
Spine curves toward raised side; ext/abd of all 4 extremities.
7-8mos → Persists
Quadruped tilting
Maintain balance w/out arms; postural adjustments
Use tilt board. Position in quadruped; raise one side.
Spine curves toward raised side; ext/abd of all 4 extremities.
9-12mos → Persists
Standing tilting
Maintain balance w/out arms; postural adjustments
Use tilt board. Position in standing; raise one side.
Spine curves toward raised side; ext/abd of all 4 extremities.
12-21 mos → Persists
Asymmetrical Tonic Neck Reflex
Babinski Reflex
Galant
Grasp Reflex
Head Righting Reflexes (Ocular and Labyrinthine Head Righting Reflexes)


Landau
Moro
Neck Righting
Parachute reflex
Symmetrical Tonic Neck Reflex

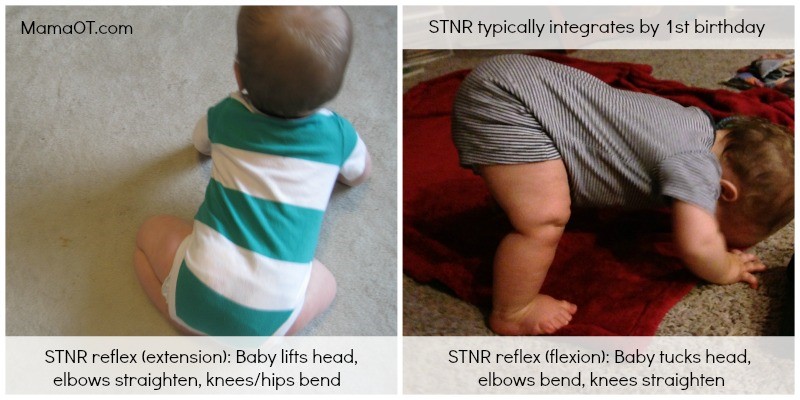
Child demonstrating an unintegrated STNR
Tonic Labyrinthe Reflex (TLR)


Sucking & Rooting
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included

