NEUROPATHIES
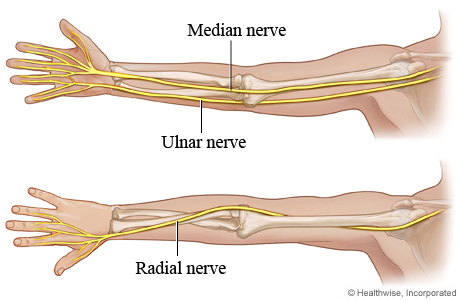
The main nerve entrapments in the upper extremity involve the median nerve, ulnar nerve, or radial nerve. The involved nerve itself may be compressed at two different levels resulting in a double crush syndrome.
As the nerves that control the upper extremity pass through the arm towards the hand, they pass through relatively fixed anatomical structures, or tunnels, usually as the nerve passes a joint. These tunnels are unable to accommodate swelling, therefore when swelling occurs within the limited volume of the tunnel, the nerve is compressed.
Common Compressive Neuropathies
Radial nerve
• Radial tunnel syndrome
• Posterior interosseous syndrome
• Superficial radial nerve syndrome
Ulnar nerve
• Cubital tunnel syndrome
• Ulnar tunnel syndrome
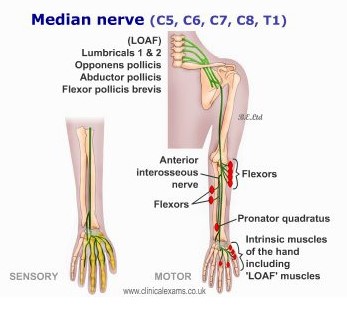
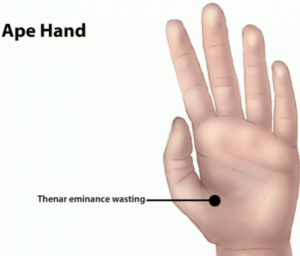
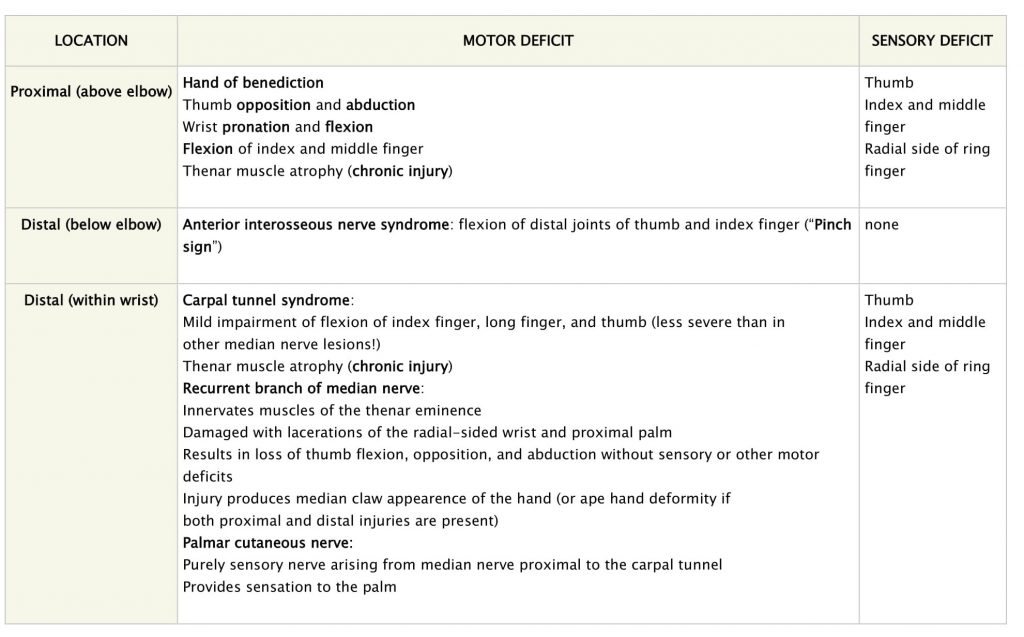
Median nerve
• Pronator syndrome
• Anterior interosseous syndrome
• Carpal tunnel syndrome
Although these differ in the anatomic distribution of their symptoms, they share a similar pathophysiology and treatment.
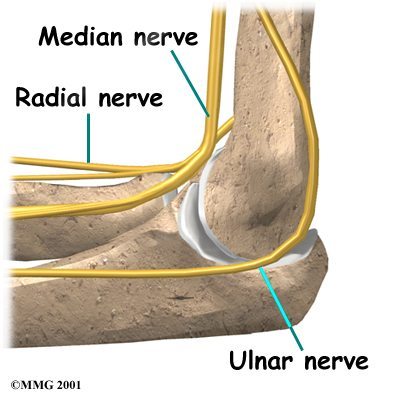
For example: Cubital and Radial Tunnels
Both pass near the elbow and run through the forearm to several fingers. The cubital tunnel houses the ulnar nerve, which winds behind and inside the elbow; the radial tunnel houses the radial nerve on the outside of the elbow. Due to the proximity of these nerves with the skin, they can be irritated by direct pressure – such as by leaning too much on the elbows or bending the arms awkwardly while asleep.
Radial Nerve 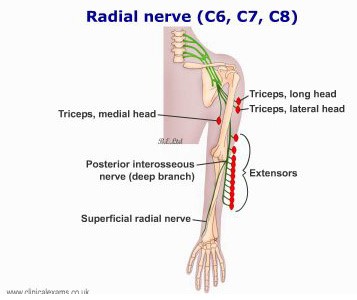
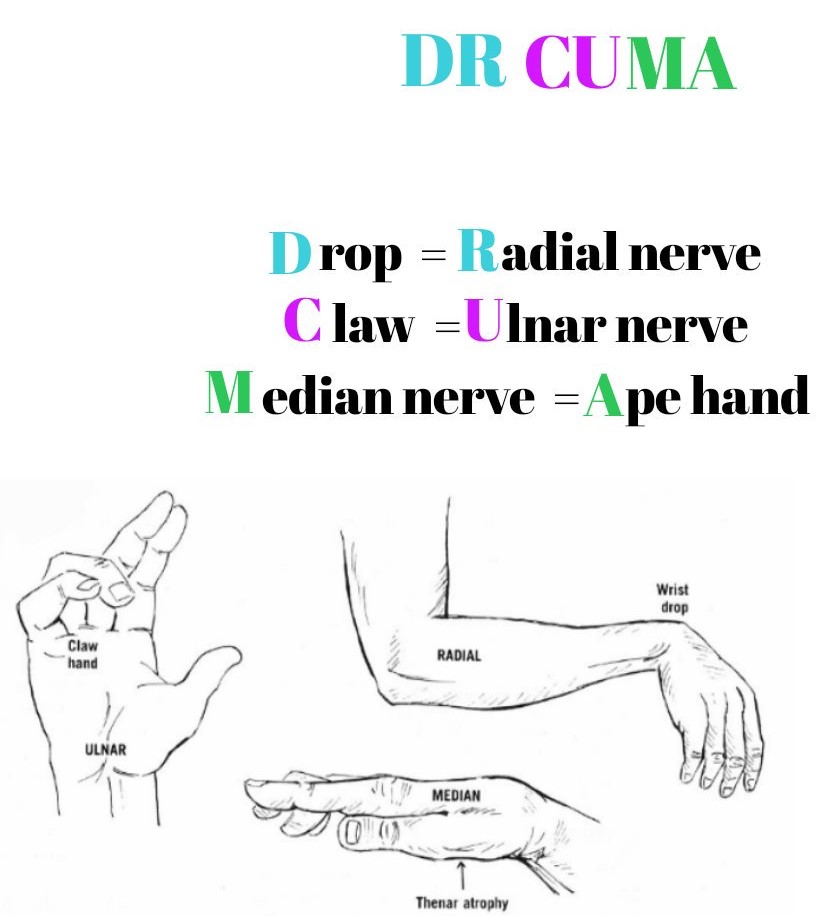
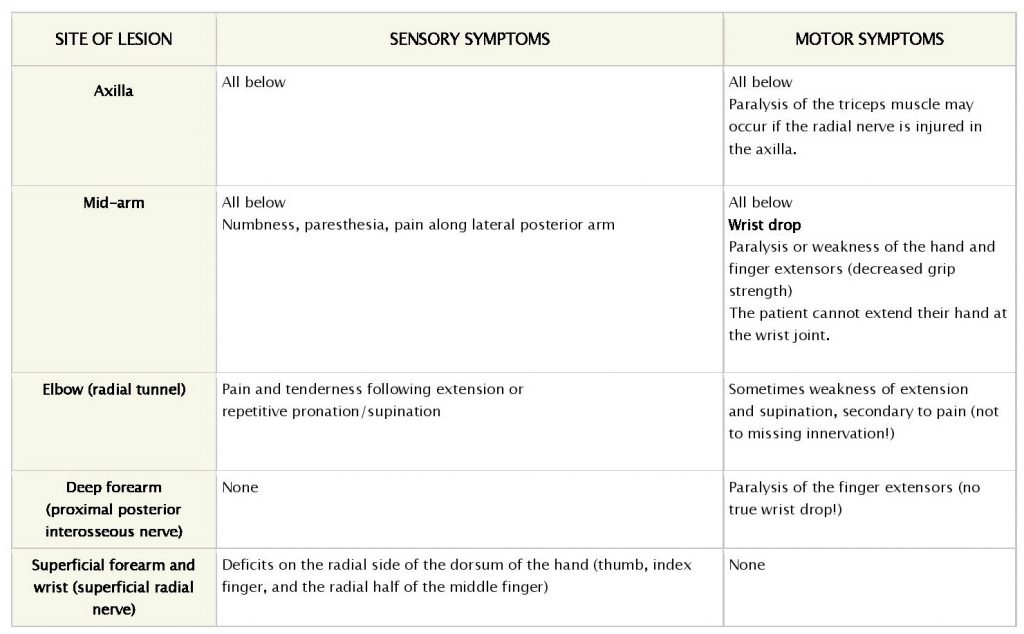
Radial neuropathies are caused by acute or chronic injury to the radial nerve. Clinical presentations vary depending on the mechanism, site, and extent of nerve injury. Radial neuropathies are characterized by sensory symptoms of pain, paresthesia, and numbness, as well as motor symptoms of weakness of extension at the elbow, wrist (“wrist drop”), and/or fingers.
Location and typical causes of injury
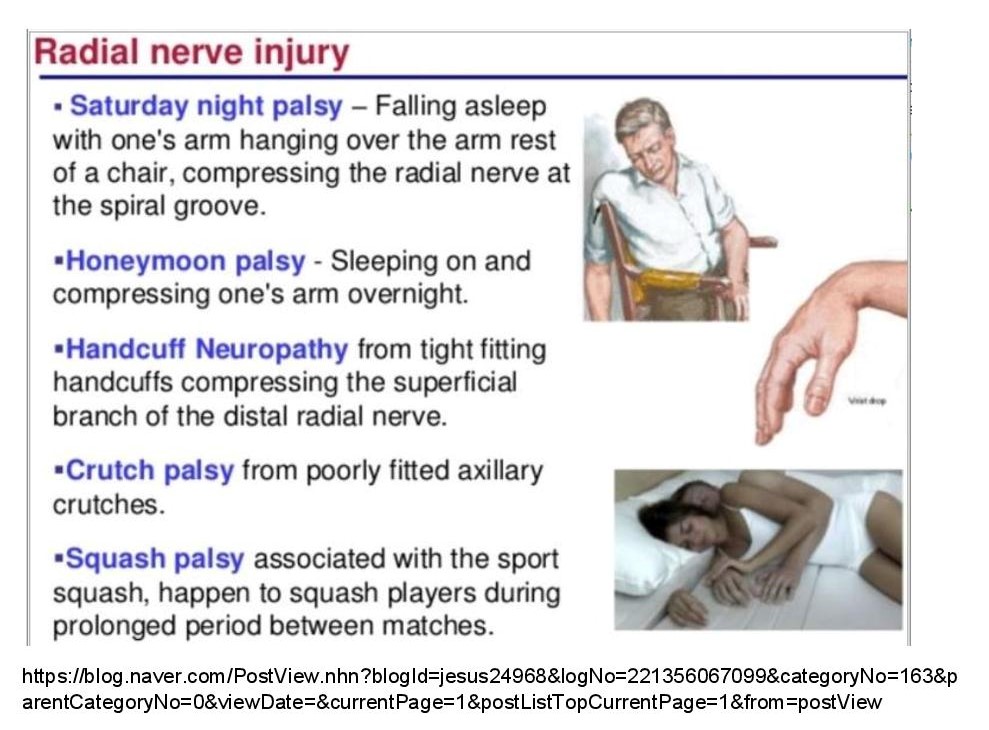
• Axilla: Improper crutch use.
• Mid-arm:
– Fracture of humerus (radial nerve runs in spiral groove).
– Compression of the radial nerve due to draping of arm over furniture (Saturday night palsy) or pressure on mid-arm; more likely in the setting of intoxication, anesthesia, or sleep (honeymoon palsy).
• Elbow: Radial tunnel syndrome due to chronic compression within the radial tunnel.
• Deep forearm: Posterior interosseous nerve syndrome (a syndrome characterized by weakness of muscles in the extensor compartment of the forearm) due to a fracture of the radial head or chronic soft tissue compression.
• Superficial forearm or wrist: Superficial radial nerve compression, called “cheiralgia paresthetica,” often due to tight wristwatches or handcuffs or repetitive pronation and supination.
Ulnar nerve 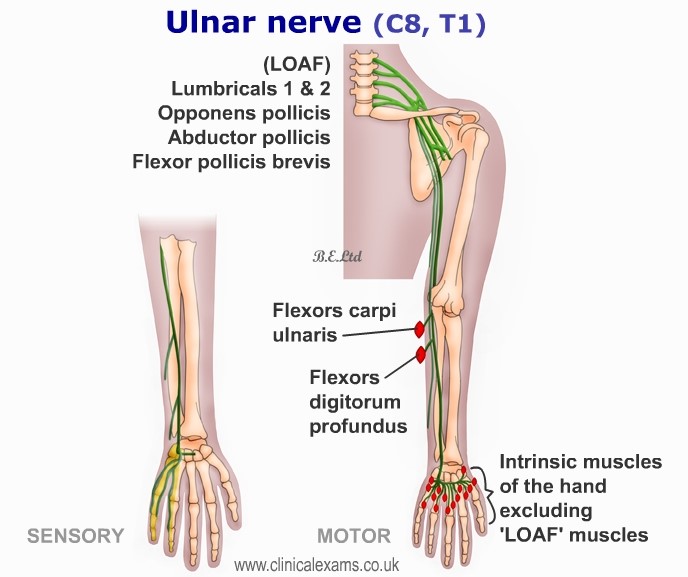
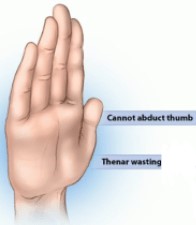
The ulnar nerve is most commonly compressed at or near the cubital tunnel of the elbow and Guyon canal of the wrist. The compression causes paresthesia, numbness, and/or pain in the ulnar nerve distribution. Depending on the site of compression, the patient may experience weakness in certain hand muscles. Ulnar entrapment neuropathy may be suspected based on clinical symptoms and signs, but it must be confirmed by electromyography (EMG).
Clinical Features:
MOTOR– Muscle weakness and atrophy.
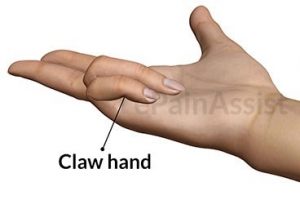
Proximal as well as distal lesions lead to claw hand deformity.
SENSORY– Sensory loss over the hypothenar eminence, ulnar 1 ½ fingers.
Lesion at the elbow: Typically presents with referred pain in the forearm. Positive Tinel test → Marked paresthesia can be reproduced in the ulnar portion of the hand by tapping on the medial epicondyle of the humerus. Tinel sign is elicited by lightly percussing along the course of the affected nerve from distal to proximal.
Lesion at the wrist: Sensory symptoms may or may not be present.