


Hand and Upper Extremity Worksheet
| Injury/Condition | Symptoms/Characteristics/ OT assessments | OT interventions e.g. ROM/Exercises/Edema control/Tendon gliding etc | Potential Splints | Contraindications | Picture |
| Adhesive tendonitis | Restricted passive shoulder range of motion; AKA frozen shoulder | PROM, modalities, encourage active use, pain management (modalities) |  |
||
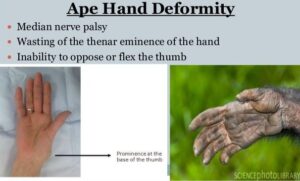
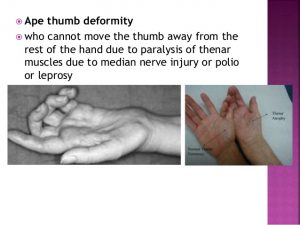
| Ape Hand | People who cannot move the thumb away from the rest of the hand. It is an inability to abduct the thumb. It is caused by either a high or low median nerve injury. If the median nerve is injured either proximally or distally, the ability to abduct and oppose the thumb will be lost due to paralysis of the thenar muscles. Ape hand deformity (simian hand), is not by itself an individual diagnosis. It is seen only after the thenar muscles have atrophied. Ape hand is the default position of the injured hand at rest. Associated symptoms: Sensory loss in index, middle, and radial side of finger; loss of pinch, thumb opposition, index finger MCP and PIP flexion; and decreased pronation (high nerve injury). |
|
|||
| Arthritis | A form of joint disorder that involves inflammation of one or more joints. Two types: OA and RA. | With a resting splint, address the natural aging process of skin and adipose tissue. Use soft straps and thick padding. | Functional splint or safe splints, depending on stage |  |
|
| Avulsion injuries | Tendon separates from the bone and its insertion and removes bone material with the tendon. (i.e. mallet finger, boutonniere deformity, swan neck deformity) |  |
|||
| Bennett’s fracture | Fracture of the first metacarpal base | Orthotics are used for immobilization as needed. ROM is begun early, within 1 week if medically cleared. A sling is used for type 1 fractures or comfort, if the patient has pain and is nervous in public places. |  |
||
| Burns | A type of injury to flesh or skin caused by heat, electricity, chemicals, friction, or radiation. Burns that affect only the superficial skin are known as superficial or first-degree burns (i.e. sunburn).
When damage penetrates into some of the underlying layers, it is a partial thickness or second-degree burn. In a full-thickness or third-degree burn, the injury extends to all layers of the skin. A fourth degree burn additionally involves injury to deeper tissues, such as muscle or bone. |
Superficial, partial thickness burns: wound care and debridement, sterile whirlpool, dressing changes, gentle A/PROM to individual’s tolerance, edema control, splinting if necessary, ADL’s and role activities.Deep partial thickness burns: wound care and debridement, sterile whirlpool, dressing changes, gentle A/PROM to individual tolerance, edema control, splinting if necessary, ADL’s and role activities, and strengthening (when wounds are healed). |
Airplane splints. Heal in anatomical position |
 |
|
| Burns to the dorsum of the hands | Passively range each digit and joint one at a time. Ranging each joint separately decreases the chance of rupturing finger extensor tendons with dorsal hand burns. | The metacarpophalangeal joints to be splinted in 70°–90° of flexion to prevent clawing of the fingers and shortening of the tendons and ligaments. This type of splint is also referred to as an antideformity splint, safe position splint, or intrinsic plus splint. Splinting the hand in the safe position allows the graft to take, the wound to heal and prevents deformities. |
 |
||
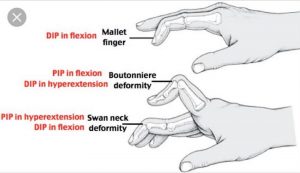
| Boutonniere deformity | PIP joint flexed, and the DIP joint hyperextended. |
Isolated DIP flexion exercises are performed. | Silver rings/ tri tip PIP is splinted in extension and isolated DIP flexion exercises are performed. |  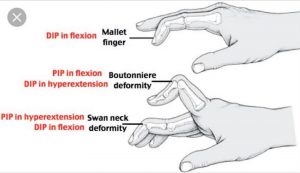 |
| Boxer’s Fracture (Proximal Fracture) |
A boxer’s fracture is the result of a clenched fist hitting an object with enough force to break the MCP neck, most commonly seen in the fourth and fifth digits. | Ulnar gutter splint | 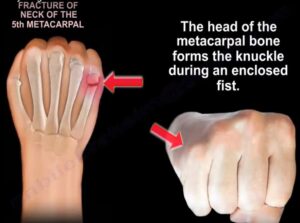 |
||
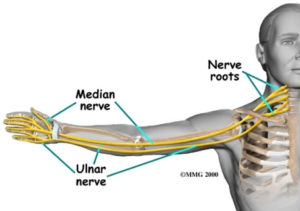
| Brachial Plexus Injury | A network of nerves that conducts signals from the spinal cord, which is housed in the spinal canal of the vertebral column (or spine), to the shoulder, arm and hand. These nerves originate in the fifth, sixth, seventh and eighth cervical (C5-C8), and first thoracic (T1) spinal nerves, and innervate the muscles and skin of the chest, shoulder, arm and hand. Brachial plexus injuries or lesions are caused by damage to those nerves. They can occur as a result of shoulder trauma, tumors, or inflammation. |
Treatment includes orthosis/splinting, surgery, or it may heal without treatment. The ability to bend the elbow (biceps function) is considered an indicator of probable recovery. Additional upward movement of the wrist and straightening of thumb and fingers an even stronger indicator of excellent spontaneous improvement. Gentle range of motion exercises. |
Flail arm splint provides the needed stability at both the shoulder and elbow for functional positioning of the hand. |
Any motion beyond 90° abduction may induce added stress to the brachial plexus and its roots. | 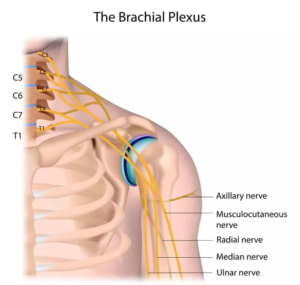 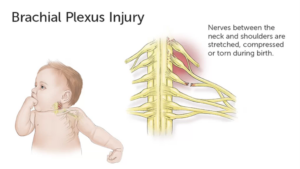 |
| C5 SCI | Movements possible: Shoulder, flexion, abduction, extension. Elbow flexion, supination. Scapular adduction, abduction. |
Wrist splint in a functional position with a slot to hold a typing stick |
 |
||
| C6-C7 SCI | Movements possible:
C6: C7: Elbow extension |
Practice to allow the proximal interphalangeal (PIP) joints to develop a contracture to facilitate functional grasp. Ranging the hand (wrist extension combined with finger flexion and wrist flexion combined with finger extension) of a patient with a spinal cord injury preserves a functional tenodesis grasp while encouraging PIP flexion contractures |
Tenodesis splint. C6 (wrist driven flexor hinge splint during a prehension activity). |
 |
|
| CMC arthritis | Most commonly involved arthritic joint in the hand. More common in women, may exist in a localized form or may exists as a systemic form of arthritis, primary form is most common in postmenopausal women, systemic form may be due to RA or gout |
A hand-based thumb splint |
 |
||
| Carpal Fracture | Fracture to the individual carpal bone. Most common injury to the wrist is the scaphoid. Lunate fractures are associated with Kienbock’s disease. |
 |
|||
| Carpal tunnel | Median nerve injury. Symptoms include palmar numbness and numbness of first digit to half of the fourth digit, with generalized weakness and pain. |
Conservative management: wrist splint in neutral, median nerve gliding exercises, activity mod, ergonomics. Post-surgical management: edema control, AROM, nerve/tendon glides, sensory re-ed., strengthening, activity mod. – Pillar pain is pain on either side of the carpal tunnel release surgery site. The source of the pain is unknown and may be ligamentous or muscular in origin. |
Wrist volar splint with wrist in neutral | 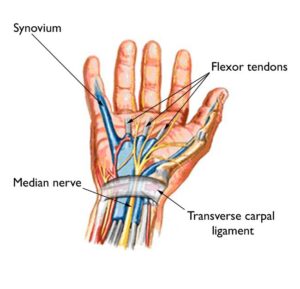 |
|
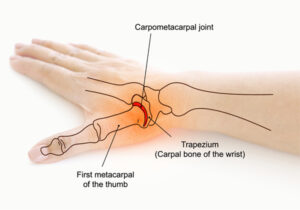
| CMC osteoarthritis | Degenerative joint disease affecting the first carpometacarpal joint (CMC1). This joint is formed by the trapezium bone of the wrist and the first metacarpal bone of the thumb. Occurs when the cushioning cartilage of the joint surfaces wear away, resulting in damage of the joint. |
Splinting and activity modification |
A thermoplastic splint osteoarthritis to support the CMC joint or a CMC neoprene wrap support to provide more movement but less support. |
 |
|
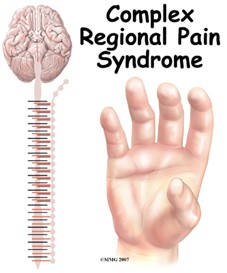
| Complex Regional Pain Syndrome (AKA: reflex sympathetic dystrophy |
Distal radius fracture is the primary reason. Pain dispropriate to an injury that is either sympathetically maintained or independent of the sympathetic nervous system. Symptoms often include pain, swelling, stiffness, sudomotor and trophic changes. |
Gentle, pain-free AROM for short periods, stress loading (i.e.scrubbing the floor, carrying a weighted bag). Pain control techniques TENS, splinting, continuous passive motion. Edema control techniques (i.e., elevation, massage AROM, contrast baths, compression). Desensitization techniques, Fluidotherapy, blocked exercises, tendon gliding, joint protection, energy conservation. Provide instruction in a stress loading program and incorporation of use of the upper extremity in functional activities. |
Static then dynamic as tolerated. Volar in extension, as tolerated Circumferential wrist might be used to avoid edema |
PROM or painful treatment. Wearing an arm sling will increase stiffness and edema because it places the extremity in a dependent and static position for long periods of time. |
 |
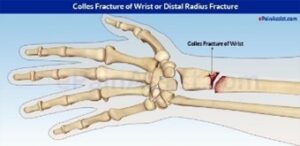
| Colles Fracture | Complete fracture of the distal radius with dorsal displacement. Most common type of wrist fracture. |
Orthotics are used for immobilization as needed. ROM is begun early, within 1 week if medically cleared. A sling is used for type 1 fractures or comfort if the patient has pain and is nervous in public places. |
  |
||
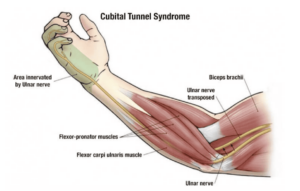
| Cubital tunnel syndrome | Ulnar nerve compression at elbow; numbness/tingling along ulnar aspect of forearm/ hand, pain at elbow with extreme , weak power grip; elbow splint to prevent ; + Tinel sign at elbow (pain or sensation) |
Conservative management: elbow pad to decrease compression of nerve, activity mod. Post-surgical management: edema control, AROM, nerve glides, strengthening, MCP splint if clawing is noted |
(non-surgical) elbow splint to prevent |
 |
|
| Cumulative trauma disorder (CTD) |
Trauma to soft tissue caused by repeated force. Patient has muscle fatigue, pain, chronic inflammation, sensory impairment, decreased ability to work. Ex. playing piano 10 hours a day |
Acute phase: reduction of inflammation and pain through static splinting, ice, contrast baths, ultrasound, interferential stimulation. Subacute phase: slow stretching, myofascial release, progressive resistive exercises as tolerated, proper body mechanics, education on identifying triggers and returning to acute phase treatment. Return to work, functional capacity evaluation, work hardening. Activity modification and proper body mechanics are essential for long-term control of an inflammatory cumulative trauma disorder. |
Static splint during activities that cause pain. |
 |
|
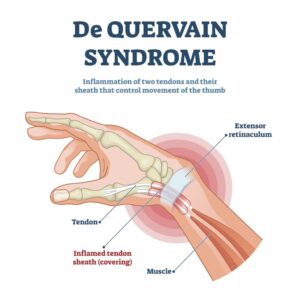
| De Quervain’s Disease | Caused by cumulative microtrauma resulting in tenosynovitis of the thumb, muscle tendon unit, abductor pollicis longus and extensor pollicis brevis, and the tendons in the first dorsal compartment of the wrist. Get it through repetition. |
Conservative management: computer ergonomics workstation education and strengthening exercises. Post-surgical management: gentle ROM, tendon gliding exercises, grip and pinch strengthening after 2 weeks, scar management and desensitization techniques are used. Use isometric exercises first. |
Thumb Spica Splint including wrist. Forearm based thumb spica splint with wrist in neutral and thumb radially abducted for 3 weeks. After 3 weeks, the patient can progress to a soft splint and isometric exercises. post-surgery put in, up to 20 degrees extension. |
Nonoperative treatment: activity modification and avoidance of pinch are recommended. |
 |
| Distal Radius fracture | Look at Colles fracture and Smith’s fracture. With edema use edema message, finger dexterity and strengthening |
Initiation of controlled AROM can begin between 3 and 6 weeks post injury if the fixation of the fracture is adequate. |
Wrist extension splint. | 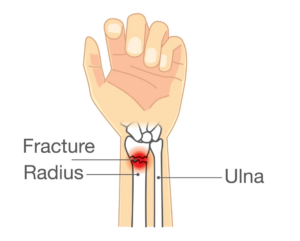 |
|
| Double Crush Syndrome | Occurs when a peripheral nerve is entrapped in more than one location. Symptoms: Intermittent diffuse arm pain and paresthesias with specific postures. | Conservative management: treat according to each nerve injury or syndrome. Nerve gliding exercises, and exercises for scapular stability, posture, and core trunk strengthening. |
Avoid movements or postures that aggravate symptoms. |
 |
|
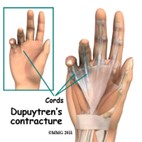
| Dupuytren’s Disease | Disease of the fascia of the palm and digits. Results in flexion deformities of the involved digits (i.e., mostly ring finger) | Wound Care: dressing changes. Whirlpool if infection is suspected. Edema Control: elevation above the heart. A/PROM and progress to strengthening when wounds are healed. Scar management, functional tasks that emphasize flexion (griping) and extension (release). |
Extension splint at all times except to remove for ROM and bathing |
 |
|
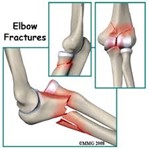
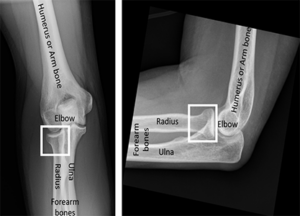
| Elbow fracture | Involvement of radial head may result in limited rotation of forearm. Usually caused by a forceful load through an outstretched arm. |
ROM begins early, within 1 week if medically cleared. | Orthotics are used for immobilization as needed. A sling is used for Type 1 fracture (nondisplaced) or comfort if the patient has pain and is nervous in public places. |
 |
|
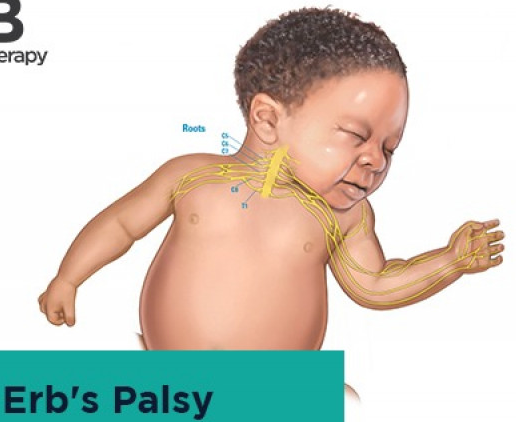
| Erb’s palsy | Paralysis of the arm caused by injury to the upper group of the arm’s main nerves, specifically the severing of the upper trunk C5–C6 nerves. The arm hangs limp with the shoulder rotated inward due to atrophy and paralysis in the biceps, deltoid, brachialis, and brachioradialis muscles. This significantly limits functional movement. |
The paralysis can either resolve on its own over a period of months, necessitate rehabilitative therapy, or require surgery |
Elbow lock splint stabilizes the elbow to enable the individual to position the hand closer to or away from his/her body for functional use. |
 |
|
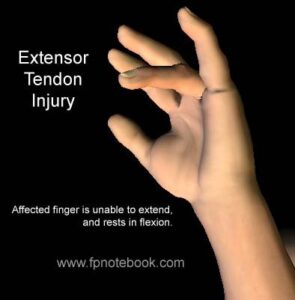
| Extensor Tendon Injury | Injury to the extensor digitorum communis, extensor indicis proprius (EIP) | Exercises promote tendon excursions and prevent adhesions. Modalities include heat, to gradually prepare the tissue for motion, and NMES to promote tendon excursion and activation. Use of modalities begins once cleared by the prescribing physician. A clearly identified and planned home program is important to ensure the patient’s safety and progress toward goals. Tendon glides are used to promote excursions and prevent adhesions. ROM. Strengthening usually not initiated until the late phase of repair, usually 8- 12 weeks after surgery. |
 |
||
| Flaccidity | Lacking firmness, resilience, or muscle tone | Resting hand splint |  |
||
| Flaccid wrist | Lacking firmness, resilience, or muscle tone in the wrist | Support the user’s wrist in 10 to 20 degrees of extension to prevent contracture, but allows digits to function |
Cock up splint |  |
|
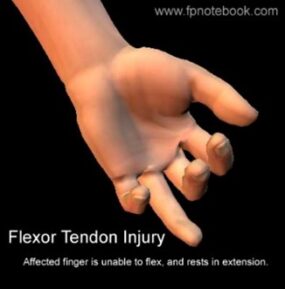
| Flexor tendon injury | A deep cut on the palm side of your fingers, hand, wrist, or forearm can damage your flexor tendons, which are the tissues that help control movement in your hand. A flexor tendon injury can make it impossible to bend your fingers or thumb. |
Flexor tendon protocol using controlled passive motion. Passive extension of the distal interphalangeal joint if the metacarpal and proximal phalangeal joints are flexed. The distal interphalangeal joint and proximal interphalangeal joint can be passively extended if the other joints of the digit are flexed to initiate tendon glide and prevent scarring of the tendon. Zone II of the flexor tendon system has been called no man’s land because excessive scarring makes it difficult to get good results from a repair. Zone IV consists of the transverse carpal ligament, and the median nerve runs under this ligament; Zone V is distal to this ligament and thus contains the median nerve branch. |
Kleinert or Duran dorsal protection splint. The dorsal blocking splint protects the surgery and guards against flexor tendon rupture. |
A tendon repair is typically, at its weakest 10–12 days post-surgery during the fibroplasia phase, in which collagen is just beginning to be laid down to strengthen the repair. |
 |
| Fracture of Medial Epicondyle | Paralyzed interossei (no abduction/adduction of the fingers) and no flexion in little and ring finger reduced causing Ulnar Claw Hand | Gentle active range-of- motion exercises may begin within 1 week after injury. | Initially, the arm should be splinted in 90° of elbow flexion. Protective splinting may be continued for 3 weeks if necessary. |
 |
|
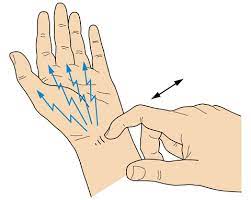
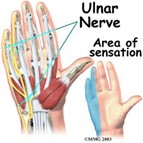
| Froment’s sign | Froment’s sign is a test of the wrist. It tests for palsy of the ulnar nerve, specifically, the action of adductor pollicis. Occurs when the flexor pollicis longus compensates for a weak or paralyzed adductor pollicis and flexor pollicis brevis. When a patient attempts to pinch, the interphalangeal joint of the thumb flexes more than usual. |
To perform the test, a patient is asked to hold an object, usually a flat object such as a piece of paper, between their thumb and index finger (pinch grip). The OT then attempts to pull the object out of the subject’s hands. A normal individual will be able to maintain a hold on the object without difficulty. However, with ulnar nerve palsy, the patient will experience difficulty maintaining a hold and will compensate by flexing the FPL (flexor pollicis longus) of the thumb to maintain grip pressure causing a pinching effect. The compensation of the affected hand results in a weak pinch grip with the tips of the thumb and index finger, therefore, with the thumb in obvious flexion. | 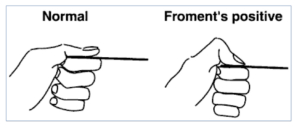 |
||
| Guyon’s canal | – An ulnar nerve compression at the wrist; numbness/tingling in ulnar nerve distribution of hand; motor weakness of ulnar nerve innervated musculature; neutral wrist splint; + Tinel’s sign at Guyon’s canal. | Conservative management: work activity mod. Post-surgical management: edema control, AROM, nerve glides, sensory reed.,strengthening | Non-surgical- wrist splint in neutral, | 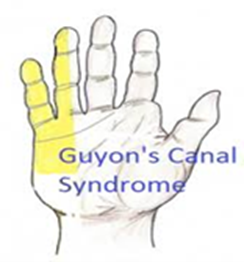 |
|
| Humeral fracture | Most common fracture of the upper arm and may involve the articular surface, greater or lesser tuberosity, or surgical neck |
With a nondisplaced fracture of the humeral neck, support from a sling and supervised exercise lead to the most desirable outcome. Displaced fractures require open reduction internal fixation surgery. Post-surgical management includes physical agent modalities for pain control, AROM, strengthening when cleared by physician. |
Humeral fracture brace for nonsurgical intervention. |  |
|
| Index finger injury | Injury to the index finger, (also referred to as forefinger, pointer finger, trigger finger, digitus secundus, digitus II, and many other terms), is the first finger and the second digit of a human hand. |
Strap incorporating the index and middle fingers provides passive rom to the index finger |
 |
||
| Intrinsic Plus Splint | Known as the safe position for hand splinting. The hand can be immobilized in this position for long periods of time without developing as much stiffness as would occur if the digits were positioned differently. |
Flexion of MPs to 90 degrees and extension at PIP and DIP. Interossei and lumbricals at their shortest. Common in patients with RA. |
 |
||
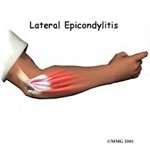
| Lateral epicondylitis | CTD from degeneration of the tendon origin as a result of repetitive microtrauma; overuse of the wrist extensors, especially the ECRB; AKA tennis elbow |
Ice/deep friction massage, stretching, activity mod, strengthening |
Elbow wrap/wrist splint. The splint rests the muscle and tendon and protects against pain with activity. |
 |
|
| Mallet Finger | Avulsion of the terminal tendon | First splint the patient’s DIP joint in full extension continuously for 6 weeks. The DIP terminal tendon is delicate and requires continuous splinting to prevent extensor lag of the tendon. |
Splinted for 6 weeks. | 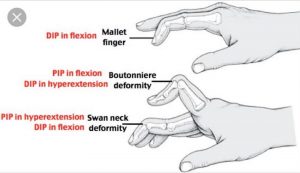 |
|
| Medial epicondylitis | same as lateral epicondylitis, but is overuse of wrist flexors; AKA golfer’s elbow |
Elbow wrap/wrist splint | 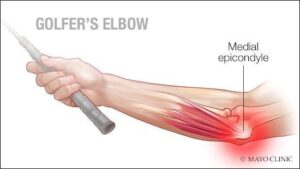 |
||
| Median Nerve Injury. | Causes ape hand deformity. Symptoms: ape hand deformity, sensory loss in index, middle, and radial side of ringer finger loss of pinch, thumb opposition,index finger MCP and PIP flexion; and decreased pronation. |
Post-surgical management: AROM and PROM in splint for digits and thumb, tendon gliding exercises, scar massage, discontinue splint at 6 weeks and begin strengthening exercises. |
Non-operative treatment: Static thenar web spacer splint. Operative treatment: dorsal wrist blocking splint worn for 4-6 weeks. |
 |
|
| Median nerve laceration | – loss of thumb opposition, weak pinch; clawing of index/mid fingers for low level lesion Ape hand- flattening of thenar eminence of Hand of benediction- loss of thumb, index, and middle fingers; high level lesion | A/PROM, scar management, strengthening, sensory re-ed |
Dorsal protection splint (30° wrist if low lesion, 90° elbow at elbow if high), C-Bar splint to prevent thumb adduction contracture |
 |
|
| Median and Ulnar nerve injury | Injury to both the median and ulnar nerves result in an impairment of function. Can be caused by car accidents and glass injuries. |
Figure of eight splint to prevent MP hyperextension or dynamic MCP flexion splint |
 |
||
| Metacarpal fracture | Ulnar gutter splint |  |
|||
| MCP flexion limitation | Difficulty flexing the MCP’s. The metacarpophalangeal joints (MCP) are of the condyloid kind, formed by the reception of the rounded heads of the metacarpal bones into shallow cavities on the proximal ends of the first phalanges, with the exception of that of the thumb, which is a hinge joint. |
The correct angle of pull for a finger loop is 90°. This angle of pull distributes the pressure most evenly to the proximal phalanx. |
 |
||
| Opponens splint | For fist contracture |  |
|||
| Pronator teres syndrome | A median nerve compression between two heads of pronator teres; symptoms same as CTS, with also aching pain in proximal volar forearm |
Elbow splint at 90° (forearm in neutral), | Avoid repetitive forearm pronation/supination |
 |
|
| Proximal Fracture | Metacarpal fracture, such as a boxer’s (4th and 5th finger) fracture |
 |
|||
| Proximal interphalangeal (PIP) flexion contracture |
A prefabricated dynamic PIP extension assist splint will improve PIP extension and takes less therapy time to fit than to custom make this splint. |
 |
|||
| Radial head fracture | 33% of elbow fractures. Usually caused by a forceful load through an outstretched arm . . |
Type 2 (displaced) treated conservatively with immobilization for 2-3 weeks and early motion with medical clearance. Type 3 (committed) treated surgically, with immobilization and early motion within the first post-surgical week as medically prescribed. |
Type 1 (nondisplaced) can be treated with a long arm sling. A Type III fracture of the radial head requires removal of the fragmented bone and a cast for 3–4 weeks to ensure proper healing and support. |
 |
|
| Radial Nerve laceration | Inability to ⁄ digits to release objects; difficulty manipulating objects |
ROM, sensory re-ed, home program, activity mod | Dynamic ⁄ splint | 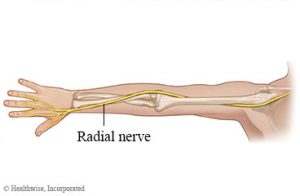 |
|
| Radial nerve palsy | Radial nerve compression; weakness/paralysis of extensors to wrist, MCPs, thumb; wrist drop; AKA Saturday night palsy. Slow nerve regeneration. |
ROM, nerve gliding, strengthening | Thumb Extension Splint, Duran dorsal protection splint, volar splint with wrist in neutral, dynamic ⁄ splint |
 |
|
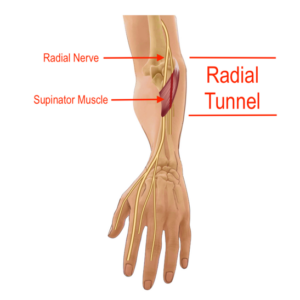
| Radial tunnel syndrome | Compression of the radial nerve in the proximal forearm resulting in a dull ache and burning sensation along the lateral forearm. | Post-surgical management: Long arm splint with the wrist in extension, elbow in flexion, and forearm in neutral rotation for 2 weeks, then wrist cock up for 2 more weeks, passive and active pronation and supination, hand strengthening exercise at 3 weeks, resistive exercise at 6 weeks. | Non-operative: Long arm orthosis with the wrist in extension, elbow in flexion, and forearm in neutral rotation, massage or TENS for pain management, pain free ROM, nerve gliding, activity modification |
Avoid forceful wrist extension and supination . |
 |
| Retts syndrome | Under the broad category of pervasive developmental disorders, together with the autism spectrum disorders. Repetitive stereotyped hand movements, such as wringing and/or repeatedly putting hands into the mouth. |
Maintain the integrity of the skin such as dynamic elbow splints that inhibit a hand to mouth pattern by limiting full elbow flexion. |  |
||
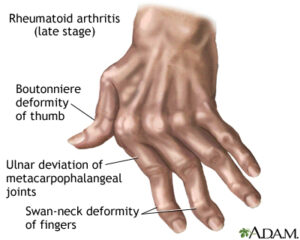
| Rheumatoid arthritis | An autoimmune disease that results in a chronic, systemic inflammatory disorder that may affect many tissues and organs, but principally attacks flexible (synovial) joints. | Volar in extension, up to 30 degrees, based on the person’s comfort level -Ulnar drift close to neutral |
 |
||
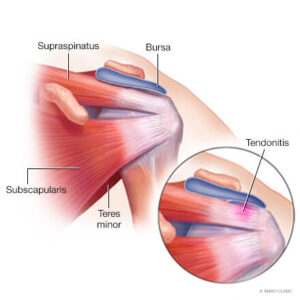
| Rotator cuff tendonitis | Inflammation (irritation and swelling) of the tendons of the shoulder | Activity mod, educate in sleeping posture (avoid arm overhead), pain management, strengthening | Codman exercises/pendulum exercises |
 |
|
| Serpentine Hand Splint | It is used when the thumb is in palmar abduction and it allows the thumb to move within abduction needed for opposition. Helps with muscle weakness for children with CP and it is important to use it during functional activities |
 |
|||
| Skier’s Thumb (Gamekeepers Thumb) | Rupture of the ulnar collateral ligament of the MCP joint of the thumb. (i.e., skiing with the thumb held in a ski pole) |
AROM and pinch strength at 6 weeks. ADL’s that require opposition and pinch strength. PROM at 8 weeks and strengthening at 10 weeks. Wear all day and night. |
Thumb splint for 4-6 weeks | Contraindicated: twisting a tight cap |   |
| Smith’s fracture | Complete fracture of the distal radius with volar displacement. |
Orthotics are used for immobilization as needed. ROM is begun early, within 1 week if medically cleared. A sling is used for type 1 fractures or comfort, if the patient has pain and is nervous in public places. |
Thumb splint | 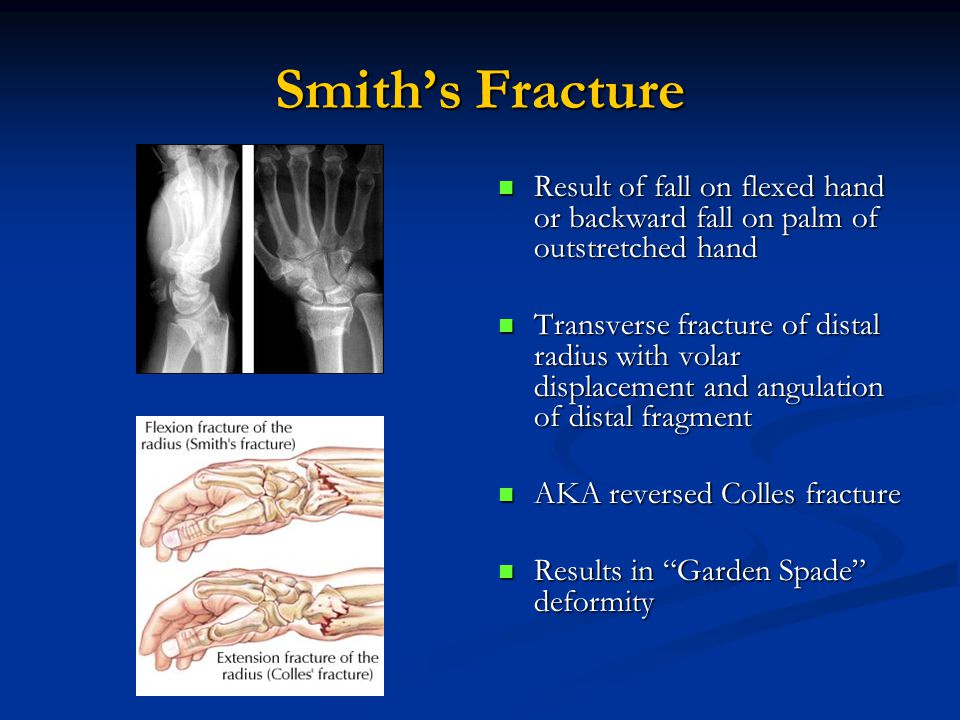
|
|
| Spasticity | Altered skeletal muscle performance in muscle tone involving hypertonia; it is also referred to as an unusual “tightness”, stiffness, or “pull” of muscles. |
Spasticity splint or cone splint |  |
||
| Swan neck deformity | Injury to the MCP, PIP, or DIP joints characterized by PIP hyperextension and DIP flexion. Adaptive equipment |
Silver rings/tripoint splint. PIP is splinted in slight flexion, or buttonhole splint |
  |
||
| Tendinitis /Tenosynovitis |
Inflammation of a tendon | Treatment is largely conservative with rest, and gradual return to exercise is a common therapy. Ice, compression and elevation. Initial recovery is typically within 2 to 3 days and full recovery is within 4 to 6 weeks. Treatment of tendinitis helps reduce some of the risks of developing tendonosis, which takes longer to heal. |
Duran dorsal protection splint, volar splint with wrist in neutral |  |
|
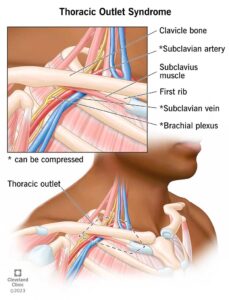
| Thoracic outlet syndrome | Excess pressure placed on a neurovascular bundle passing between the anterior scalene and middle scalene muscles |
 |
|||
| Tinel’s Sign | Tinel’s sign is a way to detect irritated nerves. It is performed by lightly tapping (percussing) over the nerve to elicit a sensation of tingling or “pins and needles” in the distribution of the nerve. The Tinel sign is typically elicited by lightly percussing along the course of the affected nerve from distal to proximal. For example, in carpal tunnel syndrome where the median nerve is compressed at the wrist, Tinel’s sign is often “positive” causing tingling in the thumb, index, middle finger and the radial half of the fourth digit. Tinel’s sign is a generalized term, and can also be positive in ulnar nerve impingement at the wrist (Guyon’s canal syndrome), where it affects the other (ulnar) half of the fourth digit and the fifth digit. |
 |
|||
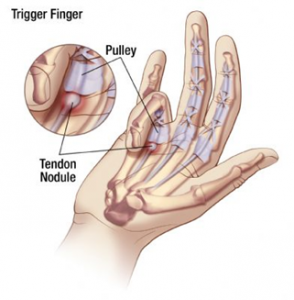
| Trigger finger | CTD; tenosynovitis of the finger flexors; most common is A1 pulley. Trigger finger is a condition in which edema in the tendon and synovium of the digit results in lack of smooth flexion or extension of the finger. | To rest the tendon and prevent snapping as the tendon pulls through the finger pulleys, the MCP joint is blocked by splinting, then gentle pull through with bending and straightening of the distal and proximal interphalangeal joints is recommended 20 times every 2 hours while the patient is awake. Edema control, tendon gliding, activity/work mod . |
Hand-based TF splint (MCP ⁄DIP and PIP is free), a splint to support the metacarpophalangeal joint in extension |
 |
|
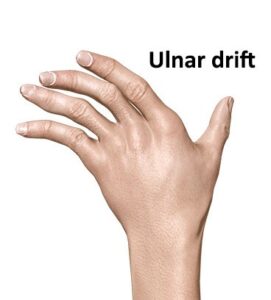
| Ulnar Drift | Hand deformity in which the swelling of the metacarpophalangeal joints (the big knuckles at the base of the fingers) causes the fingers to become displaced, tending towards the little finger. The hand, including the fingers, move towards the ulna. Ulnar deviation is a disorder in which flexion by ulnar nerve innervated muscles is intact while flexion on the median nerve side is not. |
 |
|||
| Ulnar Nerve Injury | Results in ulnar claw deformity and numbness of the ulnar side of the hand and the fifth and half of the fourth digits. See generalized weakness of the ulnar side of the hand and pain. Trouble cutting with small knife. Trouble with power grip and lateral pinch. | Orthotics are used for immobilization as needed. ROM is begun early, within 1 week if medically cleared. A sling is used for type 1 fractures or comfort if the patient has pain and is nervous in public places. |
Ulnar nerve injury splint, dynamic/static splint to position MP’s in flexion. MCP block splint. If it is a low level ulnar nerve injury, use a splint that prevents hyperextension of the MCP joints and allows MCP flexion. |
 |
|
| Upper extremity weakness | A deltoid sling . |  |
|||
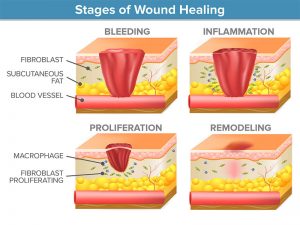
| Wound healing | Occurs in phases that generally follow the process of inflammation, proliferation, and remodeling |
 |
|||
| Wrist fracture | Injury to the wrist. The wrist is variously defined as the carpus or carpal bones, the complex of eight bones forming the proximal skeletal segment of the hand, the wrist joint or radiocarpal joint, the joint between the radius and the carpus. The wrist includes the distal parts of the bones of the forearm and the proximal parts of the five metacarpal bones. The series of joints between these bones are referred to as wrist joints. This region also includes the carpal tunnel, the anatomical snuff box, the flexor retinaculum, and the extensor retinaculum. |
Maximum passive extension up to 30 degrees. | Duran dorsal protection splint, volar splint with wrist in neutral |  |
|
| Wrist tendonitis | Inflammation of the wrist | Dexamethasone is the most widely used medication by therapists using iontophoresis because of its anti-inflammatory properties. |
 |