
DEFINITION: INCIDENCE: POSSIBLE PHYSICAL CHARACTERISTICS: Physical appearances Motor problems Other diseases Poor eyesight Poor hearing TEACHING TIPS: ATLANTOAXIAL INSTABILITY (AAI): SIGNS AND SYMPTOMS OF AAI: PRECAUTIONARY MEASURES: Information on this sheet contains only suggested guidelines. Each student must be considered individually, and in many cases, a physician’s written consent should be obtained.
DOWN SYNDROME
Down syndrome is the most common and readily identifiable chromosomal condition associated with intellectual disability. It is caused by a chromosomal abnormality; for some unexplained reason, an accident in cell development results in 47 instead of the usual 46 chromosomes. This extra chromosome changes the orderly development of the body and brain. In most cases, the diagnosis of Down syndrome is made according to results from a chromosome test generally administered shortly after birth.
• One in 1,000 live births.
• Associated with advanced maternal age, particularly if over 35 years of age.
• One in 80 infants born from women older than 40 years of age.
• Parents of any age may have a child with Down syndrome.
• Although only 5 to 8% of pregnancies occur in women over the age of 35, they account for 20% of Down syndrome births.
• There is no association between Down syndrome and any given culture, ethnic group, socioeconomic status, or geographic region.
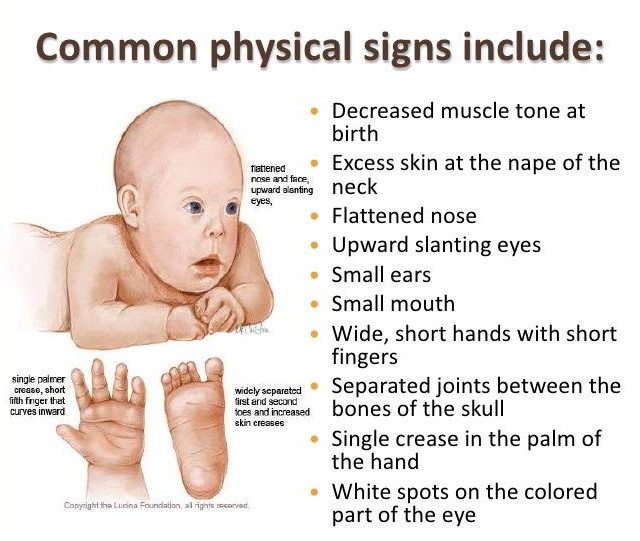
• Flat-bridged nose
• Looseness of joints
• Lack of muscle tone during infancy
• Palmer crease (a normal groove across the palm of the hand)
• Protruded abdomen
• Short fingers, limbs, and neck
• Short stature
• Slanting, almond-shaped eyes
• Small oral cavity; enlarged or protruding tongue
• Small scull
• Structural abnormalities of the lungs, nasal passages, airways and chest walls could affect breathing in strenuous exercise
• Substantial delays in reflex integration
• Tendency to be overweight
• Tendency to have atlantoaxial instability (AAI) – a misalignment of the first two cervical vertebrae of the neck French, R. (1997 – 2004)
• Varied levels of intellectual disability
• Decreased ability in kinesthetic awareness (the ability to obtain information regarding the position and movement of the body in space)
• Significant decreases in static and movement balance
• Heart disease; 40 to 60% of infants with DS have significant congenital heart disease
• Susceptibility to pulmonary problems
• Most common disorders are near sightedness and cross-eyed or squint
• Constant movement of the eyeball
• Motor problems are intensified by visual disorders
• Maybe auditory perceptual deficits – an inability to locate sound or distinguish between two sounds
• Hearing loss results in difficulty in learning to speak and follow instructions
• Adapt cardiovascular activities.
• Adapt activities involving movement on uneven surfaces.
• Adapt activities involving agility and changing directions.
• An alternative method of communication may be necessary.
• Avoid activities that place the neck in extreme flexion, such as tumbling, in individuals who test positive for AAI.
• Check medical records and follow written guidelines established by the physician.
• Coordinate with medical community to prevent contraindications.
• Discourage hyperflexible postures.
• Determine cause of problem with other health professionals.
• Encourage muscular strengthening especially around joints.
• Incorporate family into solution.
• Proper nutrition and weight control should be stressed.
• Provide calorie burning activity.
• Stress personal care (i.e., wearing weather appropriate clothing, getting enough to drink) and hygiene (washing hands and face frequently).
• Stress activities like sitting, crawling, walking, and moving through various positions to increase muscle strength.
• Teach them to move or touch particular body part.
• Utilize visual demonstrations.
• Utilize tactile demonstrations. French, R. (1997 – 2004)
• Use visual cues or stimulate visual tracking and acuity.
• Use auditory cues or require listening to complete.
Atlantoaxial Instability (AAI), also referred to as atlantoaxial subluxation, is a condition where there is increased mobility or movement between the first and second cervical vertebrae (segments of the spine in the neck). Various researchers have estimated that this condition occurs in 15% of children with Down syndrome. AAI is usually diagnosed with x-rays of the cervical spine, but typically does not produce noticeable symptoms. Symptoms are usually seen only when subluxation (incomplete or partial dislocation) of the joint between the first and second cervical vertebrae.
• Changes in bowel or bladder function
• Difficulty walking
• Weakness of any extremities
• Changes in neck posturing, neck pain, or limitations of neck movement
• Progressive clumsiness and loss of coordination
• Hypersensitivity
• Extensor plantar responses (abnormalities detected in the neurological examinations)
• Have x-rays on school file prior to participation in physical activity.
• Check medical files, speak with parents, and adhere to physician’s recommendations.
• Restrict participation in gymnastics, diving, butterfly stroke in swimming, high jump, soccer, and any warm-up exercises that places pressure on the muscles of the neck (may participate with written clearance from a physician).
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included

