People with mental health diagnoses often display certain patterns of behavior.
The following chart reviews mental health diagnoses, some of the behaviors associated with mental health conditions, and the therapeutic approaches that have been determined to be effective in addressing these behaviors.
| Description, Symptoms, and Challenges | Associated Diagnoses | Support and Treatment | Key Elements to the Therapeutic Approach and Environment | Activities | Video/Photos Example |
| An emotion that gets the body ready to fight.
Anger: strong feeling of displeasure -May manifest through physical or verbal violence, stiffening, destruction. |
-Psychotic disorder -Schizophrenia -Bipolar disorder -Psychotic depression -Organic mental disorder Some brain disorders |
• Get the patient to talk • Use your words instead of acting out • Speak to patient individually • Avoid punishing or criticizing • Instruct the patient how to correct behavior • Be direct and clear about what is expected |
• Stay a few feet away and do not face them directly • Stay out of person’s reach • Stay close to the exit • Keep the door open • Do not treat the patient alone • Remove all weapons or potential weapons • No brooms or mops |
• Journaling • Complete a feelings worksheet • Wii for boxing • Collage • Art projects – ripping magazines for pictures – have a theme for them to follow during art – projects that sequence a destructive activity followed by a constructive activity |
A woman with bipolar disorder discusses anger
|
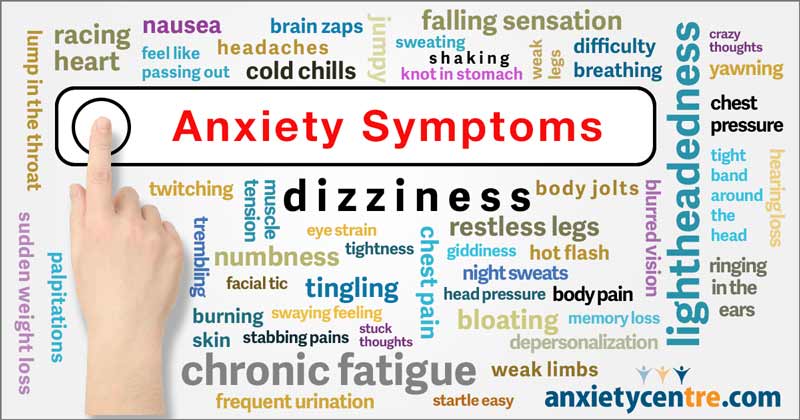
| Symptoms: Tension, nervousness, panic attacks, increased heart rate, worry, trouble sleeping, sweating, and gastrointestinal issues. A patient may feel an overwhelming sense of dread, an intense fear of death, injury, or “bad things happening”. State of tension and uneasiness that the ego is unable to resolve-Most people can control anxiety but some people cannot -Difficulty balancing fear reactions with reality-based thinking –Fear reactions may be out of proportion with the situation –Medication may be prescribed to manage anxiety |
Found in almost every diagnosis –Commonly occurs in people with depression, OCD, autism, ADHD, bipolar disorder –Psychopaths and sociopaths do not experience anxiety |
.• Talk therapy is commonly used to treat anxiety. Often if a patient can get to the root cause of their anxiety they can overcome it. • Medication to manage anxiety can also be prescribed. • Anxiety and Anxiety Disorders can also result from other, underlying medical conditions and often need to be addressed from multiple angles. • Alternative therapies such as yoga, meditation or prayer, chiropractic care, and diet and lifestyle changes are also effective in treating anxiety |
• Allow the person to express himself/herself and help him/her to learn to do it if he/she cannot. • Concentrate on productive activities. • Listen to the person’s fears. • Redirect the person’s attention to a neutral topic. • Be flexible in the response to the person’s anxiety – everyone reacts differently. – Ritualistic response: never criticize – Phobic response: encourage patients to talk about fears – Intrusive: reassure you will be available • Keep the therapy environment calm and comfortable. • Schedule therapy at a time when the clinic is not crowded. • Give the person a tour of the therapy clinic. • Provide the person with a schedule of planned therapeutic activities. • Help the person feel secure |
• Yoga. • Progressive relaxation. • Journaling with structure- helps to see antecedents. • Just right challenge. • Simple cooking tasks. • Guide patients to choose activities. • Education in diet and lifestyle changes. |
A television news anchor talks about the panic attack he had on television.
An entertaining lecture about anxiety disorders.
|
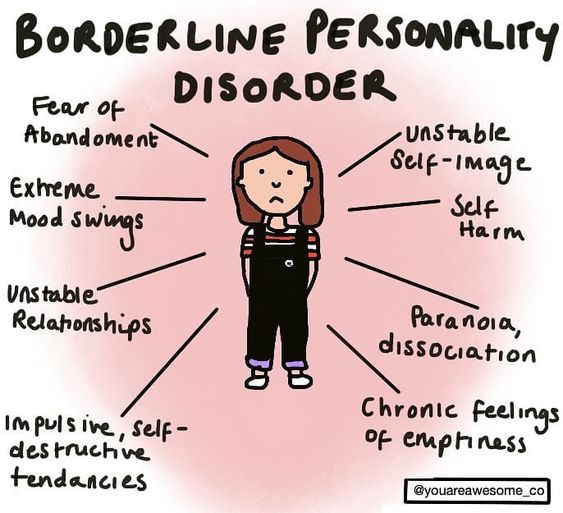
| Symptoms: –Destructive, dangerous, hostile or harmful behaviors. –Suicidal thoughts and depression –An overstated focus on self, self absorption, conceit –Difficulty building and maintaining relationships –General emotional instability –Mood swings. This is a broad disorder and can be hard to diagnose and treat. Patients are unstable and standard treatment often requires hospitalization |
– Mood disorders – Anxiety disorders – Eating disorders – Substance abuse |
Talk therapy, anger management techniques and medication are all common treatments for Borderline Personality Disorder. | The OT should make all attempts to help the patient to feel connected and included. Patients with BPD suffer from feelings of abandonment and isolation so any changes in care or setting may be unsettling. Moods can change quickly so be alert and know the signs and symptoms | • Group activities and games • Crafts and hobbies, especially familiar tasks that the patient can complete successfully • Cooking and education in nutritional food preparation • Relaxation techniques, yoga |
A celebrity rehabilitation doctor discusses borderline personality disorder
|
| Symptoms:
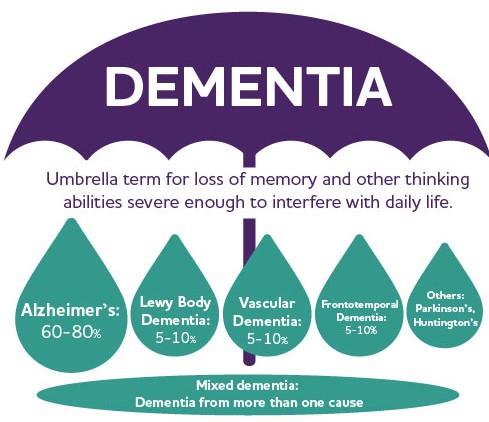
–Changes in memory, personality and habits Some changes or loss in memory is common in elderly patients but it is the combination of memory loss with other mood and behavior changes that can signal the onset of dementia. Early stage dementia: Middle Stage Dementia: Late Stage Dementia: |
– Alzheimer’s Disease – Vascular dementia – Dementia with Lewy bodies – Parkinson’s Disease – Creutzfeldt-Jacob disease – Normal pressure hydrocephalus – Huntington’s Disease – Wernicke-Korsakoff Syndrome |
While there are therapies and medications that may slow the onset of dementia, some symptoms are not treatable. Creating a dementia-friendly environment is crucial for patients. Changes may need to be made to their home, their routine, and their family or caregiver may need education and support as well. | The inevitability of dementia can lead to hopelessness, loneliness and depression in many patients. A caring, supportive, hopeful approach is key. This support may need to extend to other caregivers and family members as well. Patience is an important skill to develop when working with dementia patients. | Assistance in adapting to compensate for short term memory loss: • Set up and train in use of daily calendar or appointment book • Label cupboards and drawers with contents • Adapt home to prevent falls and safety hazards • Activities that draw upon long term memory • Familiar crafts and hobbies • Routine daily living tasks • Looking at old pictures |
A woman discusses tips for caregivers of dementia patients.
An occupational therapist works with an elderly woman with dementia. A brief overview of early stage dementia. A brief overview of middle stage dementia. A brief overview of late stage dementia. A brief overview of end stage dementia.
|
| Beliefs NOT based in reality
-Wrong idea |
–Psychotic disorder –Schizophrenia –Bipolar disorder –Eating disorders Can also occur in many other conditions. |
• Avoid discussing delusions directly • Avoid looking frustrated • Meet the patient at his or her intellectual level |
Involve the patient in real life activities | Activities should meet the patient’s intellectual capabilities • Participate in a national weekly trivia game to keep up with real life/reality based • Watching and summarizing a movie • Playing cards with friends |
A man demonstrates delusions during a counselling session
|
| Believing something to be untrue or unreal.
Refusal to face facts. We all experience denial as some point in our lives. It is a way for our minds to cope with difficult situations. However, if a patient remains in denial for too long it can keep them from being able to fully engage in treatment or therapy. Almost any diagnosis can be followed by denial. An OT needs to be ready to address it on a regular basis. Denial of a problem can force a patient to avoid treatment for a long time. |
Associated with many mental health diagnoses. May be a component of situational depression or anxiety, i.e. grief or trauma. | Denial can be a brick wall on the road to a patient’s recovery. OTs should be prepared to address it in a supportive yet direct manner. Caregivers and family members may also experience denial and may need information and education to move forward. | Denial can be overcome by continually pointing the patient back to the reality of the situation, while encouraging the patient to be hopeful. Sometimes it simply takes time to overcome denial. Often is it helpful to educate the patient on other, more effective coping mechanisms like a new activity or talk therapy. | • Relaxation and stress reduction activities • Reorientation and redirection back to reality • Adaptations to help the patient focus on coping with the new reality, reducing need for defense mechanisms |
A nurse discusses the defense mechanism of denial and gives examples.
|
| A continual and long-term sense of sadness, emptiness, despair, isolation, or hopelessness.
–May feel worthless, guilty, helpless. Depression is pervasive and can be very subtle. There can be a fine line between normal sadness and depression. Sometimes it really comes down to what characterizes the patient’s life. Do they feel sad sometimes and happy or content at other times? Or does the feeling of emptiness follow them around even when they’re doing something they love? Thankfully, depression is highly studied and there are many treatment strategies available. |
Occurs with a wide range of diagnoses –Occurs concurrently with both physical and mental health disorders –Primary symptom of affective (mood) disorder –Schizophrenia –Most personality disorders –Normal response to loss and adjustment |
Lifestyle change is considered a crucial part of depression treatment. A healthier life leads to a healthier mind. Appropriate physical activity, changes in diet, and alternative therapies have been proven to help depression. Talk therapy, support groups and medications are also helpful and often necessary. | • Allow patients to talk about themselves • Avoid being overly protective/helpful • Reinforce personal appearance • Avoid too many choices • Do not over plan • Recognize negative feelings • Notify staff of suicidal ideation • Provide a calming therapeutic environment with decreased sensory stimuli. • Increase the opportunity for decision making. • Incorporate forced choice – patient must commit to a response rather than saying “Not sure” or “It doesn’t matter”. • Match tempo- speak slowly, softly and matter of fact |
• Thought and behavior chart • Replace harmful thoughts with positive thoughts • Incorporate relaxation, tai chi or yoga • Decrease stress • Painting by numbers- with raised lines • Gross motor activity- improve depression • Sleep hygiene -Avoid naps, caffeine -Establish a bedtime routine -Encourage a sleep environment that is conducive to sleep, such as a dark, quiet room. • Involve in doing things for others – volunteer work |
A young woman describes what it is like to live with depression.
Health care professionals discuss the symptoms of depression.
|
| Abnormal eating habits.
Most commonly Anorexia, Bulimia, and Binge-Eating. Symptoms include distorted body image, fear of gaining weight, unhealthy relationship with food, excessive exercise, fasting, and induced vomiting. These behaviors lead to malnutrition and serious physical complications. |
–Depression –Anxiety –Obsessive Compulsive Disorder –Borderline personality disorder |
Many types of therapy can be helpful for patients with eating disorders. These include individual therapy, group sessions, and family therapy. Sometimes anti- depressants can also be helpful for these patients. Medical and nutritional care is also very important to the long-term health of these patients. | Eating disorders may show up along with a number of other illnesses, like depression and anxiety. A patient may develop an eating disorder as a way to control their environment or a way to punish themselves for something they feel they did wrong. Patience and empathy are crucial for OTs working with such patients. | • Therapeutic group activities • Education in nutrition, healthy weight management • Cooking activities • Relaxation and stress management • Aromatherapy • Crafts with an emphasis on creativity and messiness |
A video portrays behaviors of a person with an eating disorder.
|
| Episodic memory refers to memories of specific events or episodes. Many types of neurological disorders or trauma can have an effect on a patient’s episodic memory. Episodic memories can be categorized in two ways: visual and vocal. Each category will need to be assessed individually. |
–Alzheimer’s Disease –Senile dementia –Traumatic brain injury |
There are no known cures for episodic memory impairment. However, memory may be improved in the short term through a variety of memory-building, or brain-training activities. | When working with elderly patients it is common to observe lapses in memory but testing and assessment is needed to confirm the specific type and cause of such symptoms. | • Adaptations for memory loss, including labels on drawers and cupboards, notebooks, calendars, etc. • Memory games • Reminiscing activities using photos or stories • Familiar crafts and hobbies that the patient has participated in for a long time. |
A lecture about the hippocampus and episodic memory.
|
At the end of each month, Pass the OT awards $250 to one lucky user who fills out our brief exit survey.
This survey will be sent to you after you have taken the exam.
We look forward to helping you pass the near future
Begin ProgramPlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view this quiz
UpgradePlease upgrade your package to view full page content
UpgradePlease upgrade your package to view full page content
UpgradeWhat is included
What is not included
What is included
What is not included